{"title":"Combination of reverse shock index and simplified motor score as a strong discriminator of trauma outcomes.","authors":"Meng-Yu Wu, Giou-Teng Yiang, Ding-Kuo Chien, Sy-Jou Chen, Chi-Ming Chu, Jui-Yuan Chung, Hon-Ping Ma, Mau-Roung Lin","doi":"10.1080/07853890.2025.2458205","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The reverse shock index multiplied by simplified motor score (rSI-sMS) is a novel and rapid measure for assessing injury severity in patients with trauma in prehospital settings; however, its discriminant ability requires further validation.</p><p><strong>Methods: </strong>A retrospective cohort study was conducted from trauma database of Taipei Tzu Chi Hospital to compare the accuracy of the rSI-sMS with that of the shock index, modified shock index, reverse shock index multiplied by the Glasgow Coma Scale (rSI-GCS), and the reverse shock index multiplied by GCS motor subscale (rSI-GCSM) for discriminating in-hospital mortality, intensive care unit (ICU) admissions, prolonged ICU stays ≥14 days, and prolonged hospital stays ≥30 days in patients with trauma.</p><p><strong>Results: </strong>A total of 11,760 patients from the trauma database were included. rSI-sMS had significantly better accuracy in discriminating in-hospital mortality, ICU admissions, prolonged ICU stays (≥14 days), and prolonged hospital stays (≥30 days) than the shock index, modified shock index, and rSI-GCSM, whereas its accuracy was similar to that of the rSI-GCS. Furthermore, rSI-sMS had better accuracy for discriminating clinical outcomes in patients with an injury severity score (ISS) ≥16, motor vehicle collisions, falls, no chronic disease, and cardiovascular disease as well as in geriatric and nongeriatric patients. In patients with mixed and isolated brain injuries, rSI-sMS accurately discriminated the four clinical outcomes, similar to rSI-GCS. The optimal cutoff value of rSI-sMS had a discriminant ability of 85.0, 78.6, 75.2, and 81.0% for in-hospital mortality, ICU admissions, ICU stay ≥14 days, and hospital stays of ≥30 days, respectively.</p><p><strong>Conclusions: </strong>Compared with the shock index, modified shock index, and rSI-GCSM, rSI-sMS is a more accurate field triage scoring system for discriminating in-hospital mortality, ICU admissions, prolonged ICU stay, and prolonged hospital stays in patients with trauma.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2458205"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784069/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2025.2458205","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/29 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The reverse shock index multiplied by simplified motor score (rSI-sMS) is a novel and rapid measure for assessing injury severity in patients with trauma in prehospital settings; however, its discriminant ability requires further validation.
Methods: A retrospective cohort study was conducted from trauma database of Taipei Tzu Chi Hospital to compare the accuracy of the rSI-sMS with that of the shock index, modified shock index, reverse shock index multiplied by the Glasgow Coma Scale (rSI-GCS), and the reverse shock index multiplied by GCS motor subscale (rSI-GCSM) for discriminating in-hospital mortality, intensive care unit (ICU) admissions, prolonged ICU stays ≥14 days, and prolonged hospital stays ≥30 days in patients with trauma.
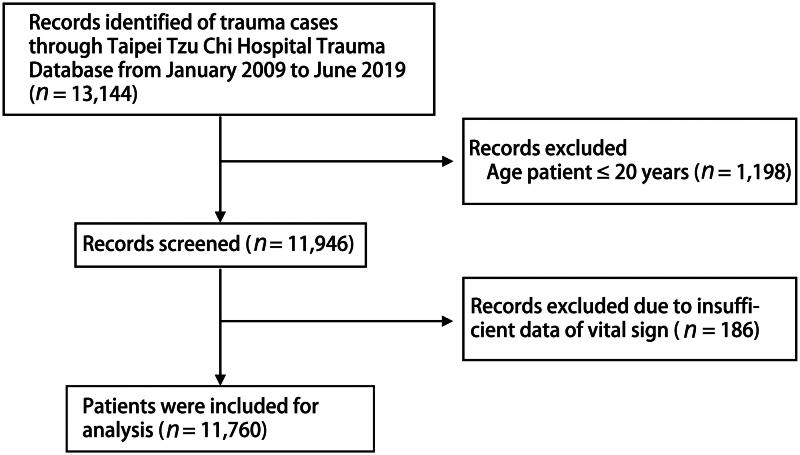
Results: A total of 11,760 patients from the trauma database were included. rSI-sMS had significantly better accuracy in discriminating in-hospital mortality, ICU admissions, prolonged ICU stays (≥14 days), and prolonged hospital stays (≥30 days) than the shock index, modified shock index, and rSI-GCSM, whereas its accuracy was similar to that of the rSI-GCS. Furthermore, rSI-sMS had better accuracy for discriminating clinical outcomes in patients with an injury severity score (ISS) ≥16, motor vehicle collisions, falls, no chronic disease, and cardiovascular disease as well as in geriatric and nongeriatric patients. In patients with mixed and isolated brain injuries, rSI-sMS accurately discriminated the four clinical outcomes, similar to rSI-GCS. The optimal cutoff value of rSI-sMS had a discriminant ability of 85.0, 78.6, 75.2, and 81.0% for in-hospital mortality, ICU admissions, ICU stay ≥14 days, and hospital stays of ≥30 days, respectively.
Conclusions: Compared with the shock index, modified shock index, and rSI-GCSM, rSI-sMS is a more accurate field triage scoring system for discriminating in-hospital mortality, ICU admissions, prolonged ICU stay, and prolonged hospital stays in patients with trauma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


