Evaluation of a peer support group programme for vulnerable host population and refugees living with diabetes and/or hypertension in Lebanon: a before-after study.
IF 3.4 2区 医学Q2 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
Leah Anku Sanga, Carla Njeim, Éimhín Ansbro, Rima Kighsro Naimi, Ali Ibrahim, Benjamin Schmid, Jasmin Lilian Diab, Jytte Roswall, Tim Clayton, Lars Bruun Larsen, Pablo Perel
{"title":"Evaluation of a peer support group programme for vulnerable host population and refugees living with diabetes and/or hypertension in Lebanon: a before-after study.","authors":"Leah Anku Sanga, Carla Njeim, Éimhín Ansbro, Rima Kighsro Naimi, Ali Ibrahim, Benjamin Schmid, Jasmin Lilian Diab, Jytte Roswall, Tim Clayton, Lars Bruun Larsen, Pablo Perel","doi":"10.1186/s13031-025-00646-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non-communicable diseases (NCDs) are the leading cause of death globally, and many humanitarian crises occur in countries with high NCD burdens. Peer support is a promising approach to improve NCD care in these settings. However, evidence on peer support for people living with NCDs in humanitarian settings is limited. We evaluated the implementation of peer support groups (PSGs) for people with diabetes and/or hypertension as part of an integrated NCD care model in four primary care centers in Lebanon.</p><p><strong>Methods: </strong>Our objectives were to: (1) evaluate the reach of the PSGs; (2) evaluate the association of PSGs with patient-reported outcomes; and (3) evaluate the association of PSGs with clinical outcomes (blood pressure, HbA1c, and BMI). We used a before-after study design and included a control group for clinical outcomes. The PSG intervention began in December 2022 and was carried out in two waves. The first wave was implemented from December 2022 to July 2023, and the second wave from July 2023 to January 2024. For the control group on clinical outcomes, we used data collected from January 2023 to January 2024. We used routinely collected programmatic and administrative data. The patient reported outcomes (PROMs) were collected at baseline and at six months by trained volunteers for all PSG participants. We performed a before-after analysis of PROMs for all patients who completed the PSG sessions. T-tests were used to analyze the differences in PROMs from baseline. Change in PROMs, together with 95% confidence intervals (CIs), and p-values for the changes were reported. To assess the association between the implementation of the PSG strategy and changes in clinical outcomes, including systolic blood pressure (SBP), glycated hemoglobin A1c (HbA1c), and body mass index (BMI), analysis of covariance (ANCOVA) models were used, adjusting for age, sex, and the baseline values of the outcome being analyzed (baseline SBP and baseline HbA1c, respectively).</p><p><strong>Results: </strong>A total of 445 patients were approached for enrolment in wave 1, 259 (58%) consented, of whom 81 were enrolled. In wave 2, 169 patients were approached, 92 (54%) consented of whom 91 were enrolled. We found some statistical evidence that PSG improved certain PROMs, including potentially clinical meaningful improvements in overall quality of life (wave 1), physical quality of life (wave 1), social quality of life (wave 2), environmental quality of life (wave 1), adherence (wave 2), patient centeredness (wave 1), and exercise (wave 1). However, we did not find strong statistical evidence of an improvement in clinical outcomes (SBP, HbA1c, or BMI) in participants of the PSGs compared to the control group. We found differences in the association of PSGs and outcomes between the two waves.</p><p><strong>Conclusion: </strong>Our study showed mixed results. In terms of reach, over 50% of those approached consented to participate. Regarding the impact on PROMs, we observed improvements in most outcomes; however we found some statistical evidence only for some. We did not find strong statistical evidence of improvement in clinical outcomes compared to the control group. Differences between the two waves may be due to differences in the populations, the way the intervention was delivered, or the individuals implementing it. Additionally, as multiple outcomes were measured, some observed differences may be due to chance. We demonstrated that it is feasible to implement PSGs in humanitarian settings and found some statistical evidence of improvement in quality of life. Further studies should assess the implementation and impact of PSGs in ways that are well accepted by local stakeholders (including humanitarian actors and people living with NCDs) and are potentially amenable to scale-up.</p>","PeriodicalId":54287,"journal":{"name":"Conflict and Health","volume":"19 1","pages":"5"},"PeriodicalIF":3.4000,"publicationDate":"2025-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11776164/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Conflict and Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13031-025-00646-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Non-communicable diseases (NCDs) are the leading cause of death globally, and many humanitarian crises occur in countries with high NCD burdens. Peer support is a promising approach to improve NCD care in these settings. However, evidence on peer support for people living with NCDs in humanitarian settings is limited. We evaluated the implementation of peer support groups (PSGs) for people with diabetes and/or hypertension as part of an integrated NCD care model in four primary care centers in Lebanon.
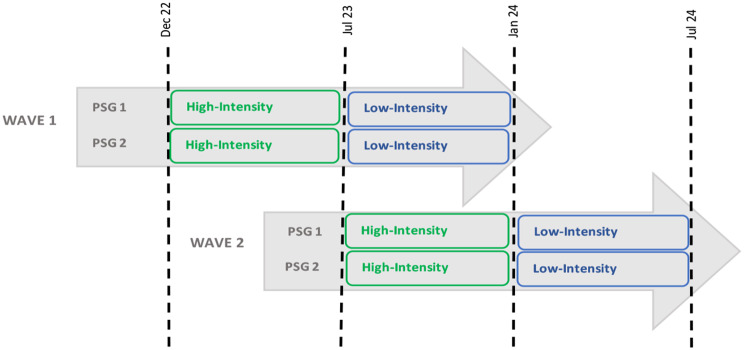
Methods: Our objectives were to: (1) evaluate the reach of the PSGs; (2) evaluate the association of PSGs with patient-reported outcomes; and (3) evaluate the association of PSGs with clinical outcomes (blood pressure, HbA1c, and BMI). We used a before-after study design and included a control group for clinical outcomes. The PSG intervention began in December 2022 and was carried out in two waves. The first wave was implemented from December 2022 to July 2023, and the second wave from July 2023 to January 2024. For the control group on clinical outcomes, we used data collected from January 2023 to January 2024. We used routinely collected programmatic and administrative data. The patient reported outcomes (PROMs) were collected at baseline and at six months by trained volunteers for all PSG participants. We performed a before-after analysis of PROMs for all patients who completed the PSG sessions. T-tests were used to analyze the differences in PROMs from baseline. Change in PROMs, together with 95% confidence intervals (CIs), and p-values for the changes were reported. To assess the association between the implementation of the PSG strategy and changes in clinical outcomes, including systolic blood pressure (SBP), glycated hemoglobin A1c (HbA1c), and body mass index (BMI), analysis of covariance (ANCOVA) models were used, adjusting for age, sex, and the baseline values of the outcome being analyzed (baseline SBP and baseline HbA1c, respectively).
Results: A total of 445 patients were approached for enrolment in wave 1, 259 (58%) consented, of whom 81 were enrolled. In wave 2, 169 patients were approached, 92 (54%) consented of whom 91 were enrolled. We found some statistical evidence that PSG improved certain PROMs, including potentially clinical meaningful improvements in overall quality of life (wave 1), physical quality of life (wave 1), social quality of life (wave 2), environmental quality of life (wave 1), adherence (wave 2), patient centeredness (wave 1), and exercise (wave 1). However, we did not find strong statistical evidence of an improvement in clinical outcomes (SBP, HbA1c, or BMI) in participants of the PSGs compared to the control group. We found differences in the association of PSGs and outcomes between the two waves.
Conclusion: Our study showed mixed results. In terms of reach, over 50% of those approached consented to participate. Regarding the impact on PROMs, we observed improvements in most outcomes; however we found some statistical evidence only for some. We did not find strong statistical evidence of improvement in clinical outcomes compared to the control group. Differences between the two waves may be due to differences in the populations, the way the intervention was delivered, or the individuals implementing it. Additionally, as multiple outcomes were measured, some observed differences may be due to chance. We demonstrated that it is feasible to implement PSGs in humanitarian settings and found some statistical evidence of improvement in quality of life. Further studies should assess the implementation and impact of PSGs in ways that are well accepted by local stakeholders (including humanitarian actors and people living with NCDs) and are potentially amenable to scale-up.
Conflict and HealthMedicine-Public Health, Environmental and Occupational Health
CiteScore
6.10
自引率
5.60%
发文量
57
审稿时长
18 weeks
期刊介绍:
Conflict and Health is a highly-accessed, open access journal providing a global platform to disseminate insightful and impactful studies documenting the public health impacts and responses related to armed conflict, humanitarian crises, and forced migration.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


