Michèle Stanciu, Joo-Young Esther Lee, Emily G McDonald, Gregory Clark, Christian A Pineau, Fares Kalache, Louis-Pierre Grenier, Évelyne Vinet, Sasha Bernatsky, Arielle Mendel
{"title":"Medication-related hospitalisations in patients with SLE.","authors":"Michèle Stanciu, Joo-Young Esther Lee, Emily G McDonald, Gregory Clark, Christian A Pineau, Fares Kalache, Louis-Pierre Grenier, Évelyne Vinet, Sasha Bernatsky, Arielle Mendel","doi":"10.1136/lupus-2024-001362","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Patients with SLE take multiple medications. Within a large prospective longitudinal SLE cohort, we characterised medication-related hospitalisations and their preventability.</p><p><strong>Methods: </strong>We identified consecutive admissions to our tertiary hospitals between 2015 and 2020. Two independent adjudicators evaluated if medication-related events contributed to the hospitalisation, considering (1) adverse drug events (ADEs) and (2) events from medication non-adherence, using the Leape and Bates method. We classified ADEs as potentially preventable/ameliorable if we identified modifiable factors. Logistic regressions with generalised estimating equations evaluated associations between participant characteristics and medication-related hospitalisations, accounting for repeat hospitalisations within the same participant.</p><p><strong>Results: </strong>We studied 68 hospitalisations among 45 participants (91% female). At first hospitalisation, the median age was 38 years (IQR 26.5-53.0) and median SLE duration was 12 years (IQR 5.5-19.5). One or more ADEs contributed to 20 (29%) hospitalisations (11/23 (48%) ADEs being preventable/ameliorable), and SLE flares associated with medication non-adherence contributed to 7 (10%) hospitalisations. Adjusting for age and sex, current prednisone use (adjusted OR (aOR) 3.7, 95% CI 1.1 to 13.0) or ≥1 current immunosuppressant (aOR 11.5, 95% CI 2.7 to 50.0), renal involvement at SLE diagnosis (aOR 6.5, 95% CI 2.7 to 15.7) and polypharmacy (≥5 medications; aOR 11.3, 95% CI 1.2 to 103.8) were associated with having an ADE-related (vs non-ADE) hospitalisation. Age at SLE diagnosis<18 years (OR 5.9, 95% CI 1.3 to 26.6) was associated with hospitalisation for a flare related to non-adherence.</p><p><strong>Conclusion: </strong>Forty per cent of SLE hospitalisations were medication-related, while half were potentially preventable/ameliorable. Renal involvement, polypharmacy, prednisone and immunosuppressant use were associated with hospitalisation related to an ADE, highlighting a vulnerable group.</p>","PeriodicalId":18126,"journal":{"name":"Lupus Science & Medicine","volume":"12 1","pages":""},"PeriodicalIF":3.5000,"publicationDate":"2025-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784163/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lupus Science & Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/lupus-2024-001362","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Patients with SLE take multiple medications. Within a large prospective longitudinal SLE cohort, we characterised medication-related hospitalisations and their preventability.
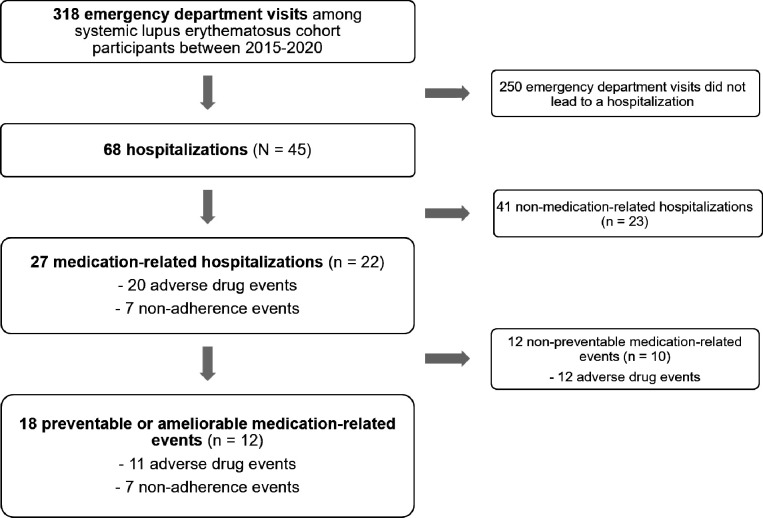
Methods: We identified consecutive admissions to our tertiary hospitals between 2015 and 2020. Two independent adjudicators evaluated if medication-related events contributed to the hospitalisation, considering (1) adverse drug events (ADEs) and (2) events from medication non-adherence, using the Leape and Bates method. We classified ADEs as potentially preventable/ameliorable if we identified modifiable factors. Logistic regressions with generalised estimating equations evaluated associations between participant characteristics and medication-related hospitalisations, accounting for repeat hospitalisations within the same participant.
Results: We studied 68 hospitalisations among 45 participants (91% female). At first hospitalisation, the median age was 38 years (IQR 26.5-53.0) and median SLE duration was 12 years (IQR 5.5-19.5). One or more ADEs contributed to 20 (29%) hospitalisations (11/23 (48%) ADEs being preventable/ameliorable), and SLE flares associated with medication non-adherence contributed to 7 (10%) hospitalisations. Adjusting for age and sex, current prednisone use (adjusted OR (aOR) 3.7, 95% CI 1.1 to 13.0) or ≥1 current immunosuppressant (aOR 11.5, 95% CI 2.7 to 50.0), renal involvement at SLE diagnosis (aOR 6.5, 95% CI 2.7 to 15.7) and polypharmacy (≥5 medications; aOR 11.3, 95% CI 1.2 to 103.8) were associated with having an ADE-related (vs non-ADE) hospitalisation. Age at SLE diagnosis<18 years (OR 5.9, 95% CI 1.3 to 26.6) was associated with hospitalisation for a flare related to non-adherence.
Conclusion: Forty per cent of SLE hospitalisations were medication-related, while half were potentially preventable/ameliorable. Renal involvement, polypharmacy, prednisone and immunosuppressant use were associated with hospitalisation related to an ADE, highlighting a vulnerable group.
期刊介绍:
Lupus Science & Medicine is a global, peer reviewed, open access online journal that provides a central point for publication of basic, clinical, translational, and epidemiological studies of all aspects of lupus and related diseases. It is the first lupus-specific open access journal in the world and was developed in response to the need for a barrier-free forum for publication of groundbreaking studies in lupus. The journal publishes research on lupus from fields including, but not limited to: rheumatology, dermatology, nephrology, immunology, pediatrics, cardiology, hepatology, pulmonology, obstetrics and gynecology, and psychiatry.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


