Ahmad Jradi, Kaline Maya Khoury, Karam Karam, Dr Ihab I El Hajj, Elias Fiani
{"title":"Lymphocytic Esophagitis: Navigating an Uncharted Territory.","authors":"Ahmad Jradi, Kaline Maya Khoury, Karam Karam, Dr Ihab I El Hajj, Elias Fiani","doi":"10.1177/23247096251313734","DOIUrl":null,"url":null,"abstract":"<p><p>Lymphocytic esophagitis (LE) is an uncommon subtype of esophagitis defined by persistent esophageal inflammation characterized by a high count of intraepithelial lymphocytes with scarce granulocytes. Although LE can present with atypical features such as chest pain, its clinical presentation can mimic that of gastroesophageal reflux disease or eosinophilic esophagitis, highlighting the importance of biopsy in diagnosing LE. Studies are still limited in understanding the pathophysiology behind this disease warranting further research. A 47-year-old female patient sought medical care with a chief complaint of recurrent substernal chest pain for the past year. An esophagogastroduodenoscopy was performed and showed patchy linear esophageal erosions and mucosal edema in the middle third of the esophagus with mild erythema. Biopsies revealed intraepithelial lymphocytosis with more than 40 lymphocytes per high-power field, corroborating a diagnosis of LE. Patient reported improvement after receiving high dose of proton pump inhibitor (PPI) on her first follow-up, advised to follow a low-acid diet and an annual endoscopy to monitor her response to treatment. Lymphocytic esophagitis often presents with symptoms that overlap with other esophageal diseases explaining the possible errors in underdiagnosing it as reason behind non-cardiac chest pain. This case plays an instrumental role in changing the way physicians translate unexplained chest pain, adding LE to their list of differential diagnosis as prompt detection slows us to start management with PPIs quicker and lessen the burden of symptoms on the patient. Standardized treatment approaches and further studies are required to clarify the connection between LE and non-cardiac chest discomfort.</p>","PeriodicalId":16198,"journal":{"name":"Journal of investigative medicine high impact case reports","volume":"13 ","pages":"23247096251313734"},"PeriodicalIF":0.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11783483/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of investigative medicine high impact case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23247096251313734","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
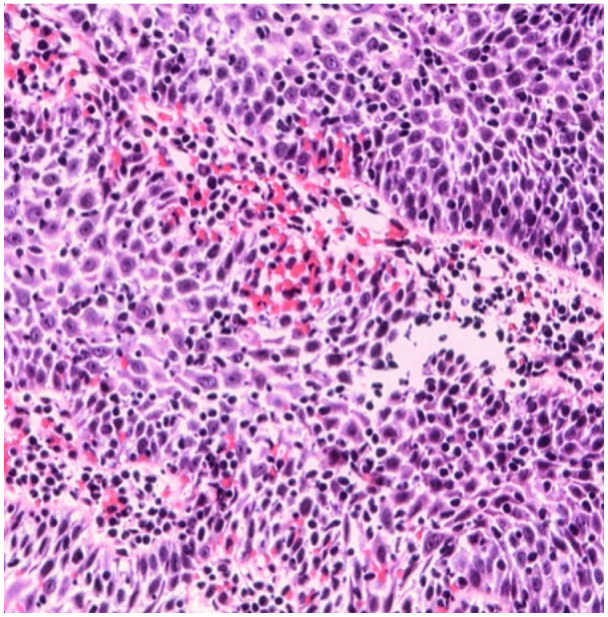
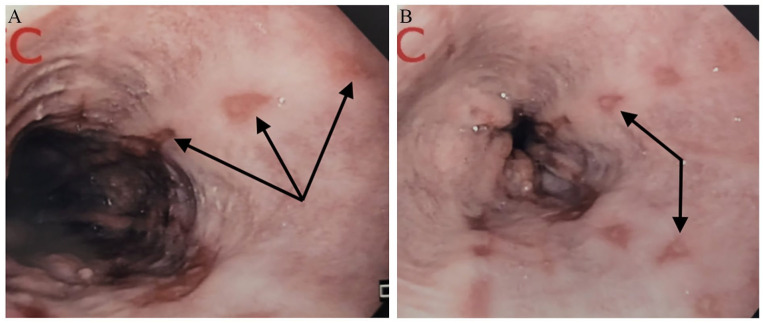
Lymphocytic esophagitis (LE) is an uncommon subtype of esophagitis defined by persistent esophageal inflammation characterized by a high count of intraepithelial lymphocytes with scarce granulocytes. Although LE can present with atypical features such as chest pain, its clinical presentation can mimic that of gastroesophageal reflux disease or eosinophilic esophagitis, highlighting the importance of biopsy in diagnosing LE. Studies are still limited in understanding the pathophysiology behind this disease warranting further research. A 47-year-old female patient sought medical care with a chief complaint of recurrent substernal chest pain for the past year. An esophagogastroduodenoscopy was performed and showed patchy linear esophageal erosions and mucosal edema in the middle third of the esophagus with mild erythema. Biopsies revealed intraepithelial lymphocytosis with more than 40 lymphocytes per high-power field, corroborating a diagnosis of LE. Patient reported improvement after receiving high dose of proton pump inhibitor (PPI) on her first follow-up, advised to follow a low-acid diet and an annual endoscopy to monitor her response to treatment. Lymphocytic esophagitis often presents with symptoms that overlap with other esophageal diseases explaining the possible errors in underdiagnosing it as reason behind non-cardiac chest pain. This case plays an instrumental role in changing the way physicians translate unexplained chest pain, adding LE to their list of differential diagnosis as prompt detection slows us to start management with PPIs quicker and lessen the burden of symptoms on the patient. Standardized treatment approaches and further studies are required to clarify the connection between LE and non-cardiac chest discomfort.
期刊介绍:
The AFMR is committed to enhancing the training and career development of our members and to furthering its mission to facilitate the conduct of research to improve medical care. Case reports represent an important avenue for trainees (interns, residents, and fellows) and early-stage faculty to demonstrate productive, scholarly activity.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


