Jessica Pearce, Sally Martin, Sophie Heritage, Emma G Khoury, Joanna Kucharczak, Thitikorn Nuamek, David A Cairns, Galina Velikova, Suzanne H Richards, Andrew Clegg, Alexandra Gilbert
{"title":"Frailty and outcomes in adults undergoing systemic anticancer treatment: a systematic review and meta-analysis.","authors":"Jessica Pearce, Sally Martin, Sophie Heritage, Emma G Khoury, Joanna Kucharczak, Thitikorn Nuamek, David A Cairns, Galina Velikova, Suzanne H Richards, Andrew Clegg, Alexandra Gilbert","doi":"10.1093/jnci/djaf017","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>It is increasingly recognized that frailty should be assessed and considered in treatment decision making in patients with cancer. This review and meta-analysis synthesizes existing evidence evaluating the association between baseline frailty and systemic anticancer treatment outcomes in adults with cancer.</p><p><strong>Methods: </strong>Five databases were systematically searched from database inception to January 2023 to identify prognostic factor studies (cohort or case-control design) reporting the associations between validated frailty assessments (pretreatment) and follow-up outcomes in adults with solid-organ malignancy undergoing systemic anticancer treatment. Risk of bias was assessed via Quality of Prognosis Studies in Systematic Reviews tool. Where appropriate, associations between frailty and outcomes (survival, toxicity, treatment tolerance, functional decline/quality of life, and hospitalization) were synthesized in meta-analysis and presented as forest plots.</p><p><strong>Results: </strong>A total of 58 studies met inclusion criteria. They were undertaken in a range of tumor sites and mainly in older patients and advanced and/or palliative disease settings. Most had low or moderate risk of bias. Nine frailty assessment tools were evaluated. Four outcomes were synthesized in meta-analysis, which demonstrated the prognostic value of 2 tools: Geriatric-8 (survival, treatment tolerance, hospitalization) and Vulnerable Elders Survey-13 (survival, toxicity, treatment tolerance). Overall pooled estimates indicate that frailty conveys an increased risk of mortality (hazard ratio [HR] = 1.68, 95% confidence interval [CI] = 1.41 to 2.00), toxicity (odds ratio [OR] 1.83, 95% CI = 1.24 to 2.68), treatment intolerance (OR = 1.68, 95% CI = 1.32 to 2.12), and hospitalization (OR = 1.94, 95% CI = 1.32 to 2.83).</p><p><strong>Conclusion: </strong>Simple, brief frailty assessments including Geriatric-8 and Vulnerable Elders Survey-13 are prognostic for a range of important outcomes in patients undergoing systemic anticancer treatment. Risk estimates should be used to support shared decision making.</p>","PeriodicalId":14809,"journal":{"name":"JNCI Journal of the National Cancer Institute","volume":" ","pages":"1316-1339"},"PeriodicalIF":7.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12232047/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JNCI Journal of the National Cancer Institute","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/jnci/djaf017","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: It is increasingly recognized that frailty should be assessed and considered in treatment decision making in patients with cancer. This review and meta-analysis synthesizes existing evidence evaluating the association between baseline frailty and systemic anticancer treatment outcomes in adults with cancer.
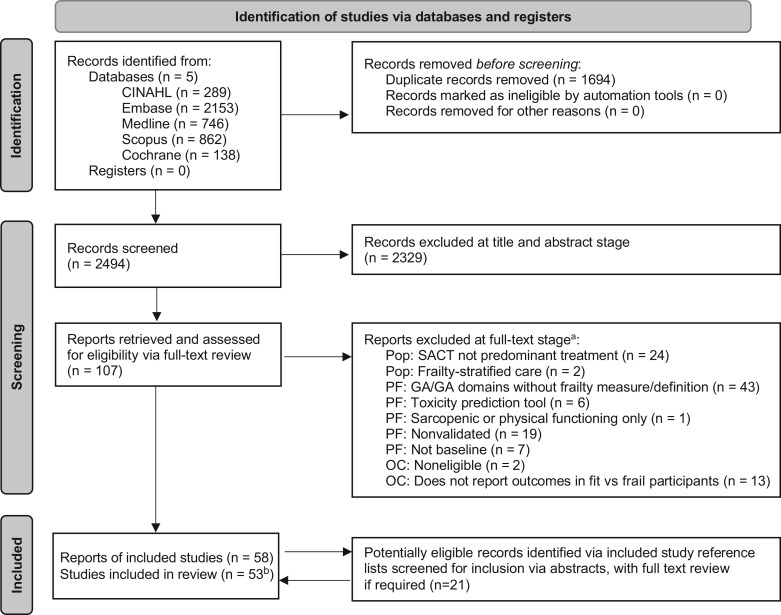
Methods: Five databases were systematically searched from database inception to January 2023 to identify prognostic factor studies (cohort or case-control design) reporting the associations between validated frailty assessments (pretreatment) and follow-up outcomes in adults with solid-organ malignancy undergoing systemic anticancer treatment. Risk of bias was assessed via Quality of Prognosis Studies in Systematic Reviews tool. Where appropriate, associations between frailty and outcomes (survival, toxicity, treatment tolerance, functional decline/quality of life, and hospitalization) were synthesized in meta-analysis and presented as forest plots.
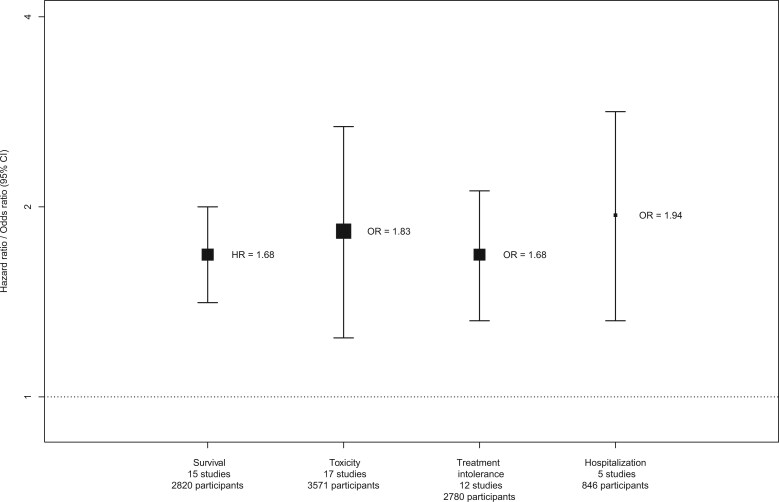
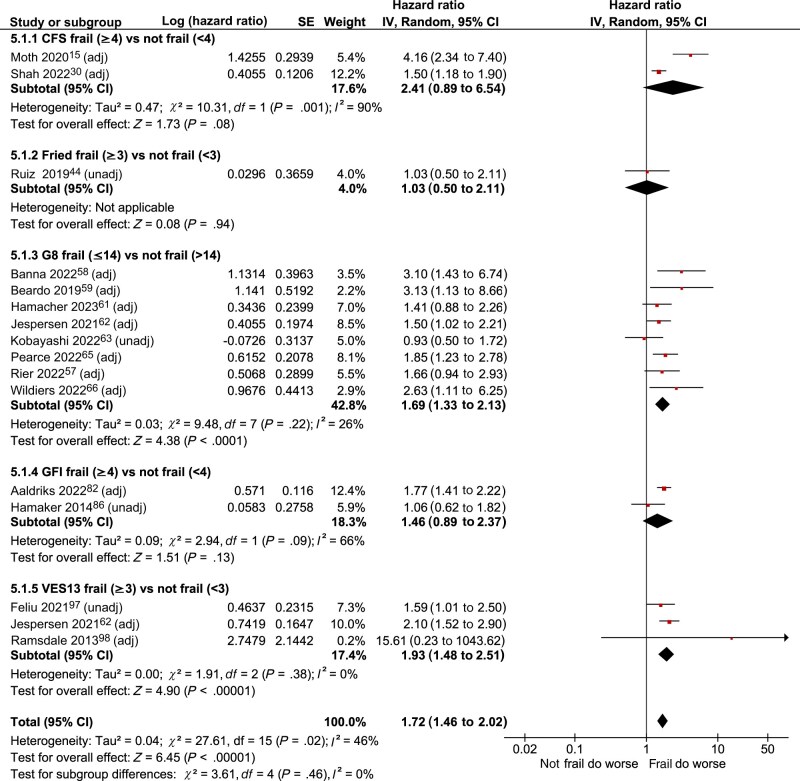
Results: A total of 58 studies met inclusion criteria. They were undertaken in a range of tumor sites and mainly in older patients and advanced and/or palliative disease settings. Most had low or moderate risk of bias. Nine frailty assessment tools were evaluated. Four outcomes were synthesized in meta-analysis, which demonstrated the prognostic value of 2 tools: Geriatric-8 (survival, treatment tolerance, hospitalization) and Vulnerable Elders Survey-13 (survival, toxicity, treatment tolerance). Overall pooled estimates indicate that frailty conveys an increased risk of mortality (hazard ratio [HR] = 1.68, 95% confidence interval [CI] = 1.41 to 2.00), toxicity (odds ratio [OR] 1.83, 95% CI = 1.24 to 2.68), treatment intolerance (OR = 1.68, 95% CI = 1.32 to 2.12), and hospitalization (OR = 1.94, 95% CI = 1.32 to 2.83).
Conclusion: Simple, brief frailty assessments including Geriatric-8 and Vulnerable Elders Survey-13 are prognostic for a range of important outcomes in patients undergoing systemic anticancer treatment. Risk estimates should be used to support shared decision making.
期刊介绍:
The Journal of the National Cancer Institute is a reputable publication that undergoes a peer-review process. It is available in both print (ISSN: 0027-8874) and online (ISSN: 1460-2105) formats, with 12 issues released annually. The journal's primary aim is to disseminate innovative and important discoveries in the field of cancer research, with specific emphasis on clinical, epidemiologic, behavioral, and health outcomes studies. Authors are encouraged to submit reviews, minireviews, and commentaries. The journal ensures that submitted manuscripts undergo a rigorous and expedited review to publish scientifically and medically significant findings in a timely manner.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


