{"title":"Implementation of a clinical pathway for diabetes-related foot ulcers reduced the number of amputations and shortened hospital stay.","authors":"Monica Sailer, Hilde Wergeland, Per-Henrik Randsborg","doi":"10.1002/jfa2.70024","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Diabetes-related foot ulcer (DFU) is the leading cause for lower extremity amputations (LEAs) in western countries, and may cause social isolation, depression, and death. However, people with DFU are not offered the same prioritized care as cancer patients, despite comparable mortality rates. We therefore decided to create a clinical pathway for patients with DFU. The purpose of this study is to evaluate the efficacy of implementing a new clinical pathway on rates of LEA, length of hospital stays, and cost reduction.</p><p><strong>Methods: </strong>On January 1, 2019, a new clinical pathway ensured that all patients with a DFU were evaluated in a designated clinic run by a foot and ankle orthopedic surgeon in collaboration with the vascular surgeons, supported by a specialized wound nurse and a certified prosthetist/orthotist (CPO). We designed an algorithm for the first consultation to identify patients in need for further investigation by other specialties such as endocrinology, infectious diseases, cardiology, or vascular surgery. All patients underwent a surgical wound debridement of DFU. Negative pressure wound therapy (NPWT) was not applied. After surgery, the dressings were changed daily on the ward, until the wound was deemed viable and clean. The patients were followed for two years and compared to a historic cohort of patients with DFU admitted to the institution in 2017.</p><p><strong>Results: </strong>The number of major amputations was reduced from 65% (13/20) to 7.4% (2/27) (p < 0.001) after the introduction of the clinical pathway. Both the mean number of surgical revisions (5.5 vs. 1.2) and the median length of stay (46 vs. 9 days) were statistically significantly reduced. The median cost per patient was reduced by 76% (from €538 000 to €129 000, p < 0.001).</p><p><strong>Conclusion: </strong>The clinical pathway for managing DFUs resulted in a reduction in major amputations and shorter hospital stays. Discontinuing NPWT after surgical debridement did not adversely affect clinical outcomes. The new pathway also contributed to lower healthcare costs.</p>","PeriodicalId":49164,"journal":{"name":"Journal of Foot and Ankle Research","volume":"18 1","pages":"e70024"},"PeriodicalIF":2.2000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11774619/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Foot and Ankle Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/jfa2.70024","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Diabetes-related foot ulcer (DFU) is the leading cause for lower extremity amputations (LEAs) in western countries, and may cause social isolation, depression, and death. However, people with DFU are not offered the same prioritized care as cancer patients, despite comparable mortality rates. We therefore decided to create a clinical pathway for patients with DFU. The purpose of this study is to evaluate the efficacy of implementing a new clinical pathway on rates of LEA, length of hospital stays, and cost reduction.
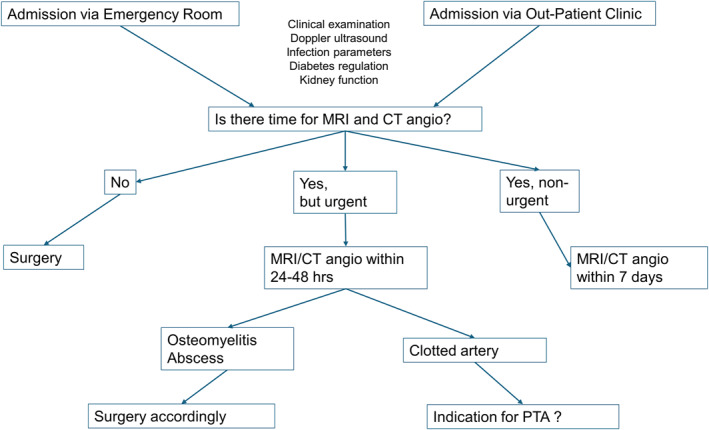
Methods: On January 1, 2019, a new clinical pathway ensured that all patients with a DFU were evaluated in a designated clinic run by a foot and ankle orthopedic surgeon in collaboration with the vascular surgeons, supported by a specialized wound nurse and a certified prosthetist/orthotist (CPO). We designed an algorithm for the first consultation to identify patients in need for further investigation by other specialties such as endocrinology, infectious diseases, cardiology, or vascular surgery. All patients underwent a surgical wound debridement of DFU. Negative pressure wound therapy (NPWT) was not applied. After surgery, the dressings were changed daily on the ward, until the wound was deemed viable and clean. The patients were followed for two years and compared to a historic cohort of patients with DFU admitted to the institution in 2017.
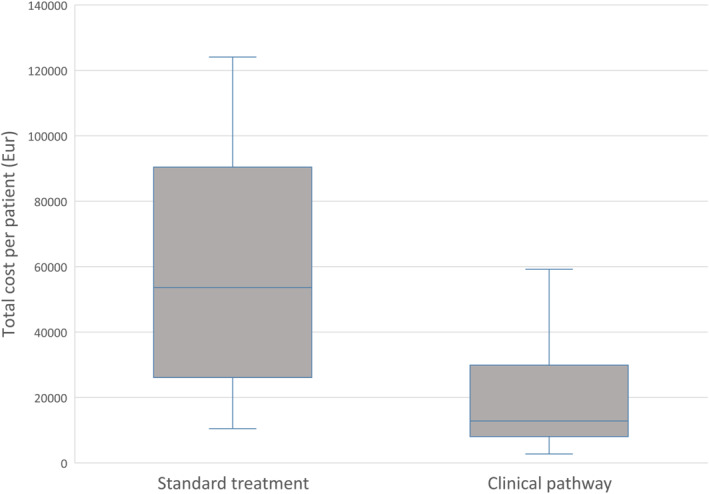
Results: The number of major amputations was reduced from 65% (13/20) to 7.4% (2/27) (p < 0.001) after the introduction of the clinical pathway. Both the mean number of surgical revisions (5.5 vs. 1.2) and the median length of stay (46 vs. 9 days) were statistically significantly reduced. The median cost per patient was reduced by 76% (from €538 000 to €129 000, p < 0.001).
Conclusion: The clinical pathway for managing DFUs resulted in a reduction in major amputations and shorter hospital stays. Discontinuing NPWT after surgical debridement did not adversely affect clinical outcomes. The new pathway also contributed to lower healthcare costs.
期刊介绍:
Journal of Foot and Ankle Research, the official journal of the Australian Podiatry Association and The College of Podiatry (UK), is an open access journal that encompasses all aspects of policy, organisation, delivery and clinical practice related to the assessment, diagnosis, prevention and management of foot and ankle disorders.
Journal of Foot and Ankle Research covers a wide range of clinical subject areas, including diabetology, paediatrics, sports medicine, gerontology and geriatrics, foot surgery, physical therapy, dermatology, wound management, radiology, biomechanics and bioengineering, orthotics and prosthetics, as well the broad areas of epidemiology, policy, organisation and delivery of services related to foot and ankle care.
The journal encourages submissions from all health professionals who manage lower limb conditions, including podiatrists, nurses, physical therapists and physiotherapists, orthopaedists, manual therapists, medical specialists and general medical practitioners, as well as health service researchers concerned with foot and ankle care.
The Australian Podiatry Association and the College of Podiatry (UK) have reserve funds to cover the article-processing charge for manuscripts submitted by its members. Society members can email the appropriate contact at Australian Podiatry Association or The College of Podiatry to obtain the corresponding code to enter on submission.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


