{"title":"Finerenone: Will It Be a Game-changer?","authors":"Dinesh Khullar, Anish Kumar Gupta, Kulwant Singh","doi":"10.15420/cfr.2024.11","DOIUrl":null,"url":null,"abstract":"<p><p>Heart failure (HF) is a major contributor to hospitalisations and accounts for 7% of cardiovascular-related deaths, with patients who have chronic kidney disease and type 2 diabetes at heightened risk. Existing treatment guidelines inadequately address these comorbidities. Steroidal mineralocorticoid receptor antagonists (MRAs) are commonly used in HF with reduced ejection fraction but pose risks, such as hyperkalaemia and acute kidney injury. Finerenone, a non-steroidal MRA, offers a safer alternative, with higher selectivity, reduced electrolyte disturbances and beneficial effects on heart and kidney tissues. Preclinical studies show anti-inflammatory and anti-fibrotic effects, while phase III trials (ARTS and ARTS-HF) demonstrated fewer hyperkalaemia incidents compared with spironolactone. In phase III trials (FIDELIO-DKD and FIGARO-DKD), finerenone reduced HF hospitalisations by 22% in patients with chronic kidney disease and type 2 diabetes. The FINEARTS-HF trial found that finerenone significantly reduced the risk of worsening HF events or CV death in patients with HF with mildly reduced or preserved ejection fraction. Its combination with therapies, such as sodium-glucose cotransporter 2 inhibitors, shows promise and ongoing trials, such as REDEFINE-HF, FINALITY-HF and CONFIRMATION-HF, are investigating its efficacy in other HF phenotypes. These studies will further establish the role of finerenone in managing cardio-renal-metabolic diseases.</p>","PeriodicalId":33741,"journal":{"name":"Cardiac Failure Review","volume":"10 ","pages":"e19"},"PeriodicalIF":5.7000,"publicationDate":"2024-12-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11770532/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiac Failure Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/cfr.2024.11","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
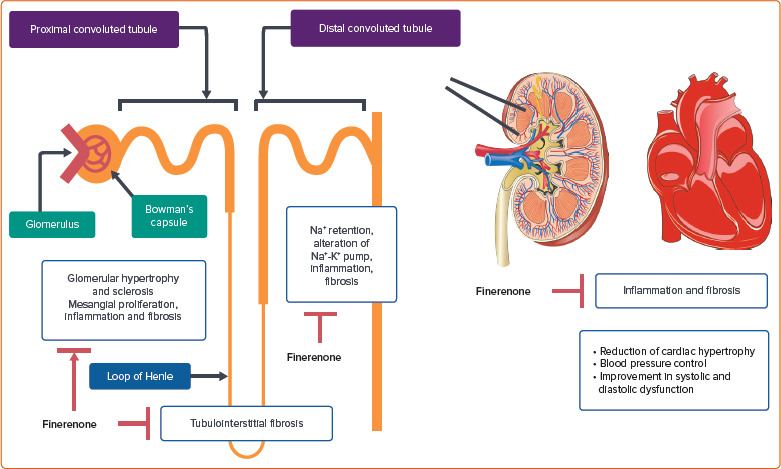
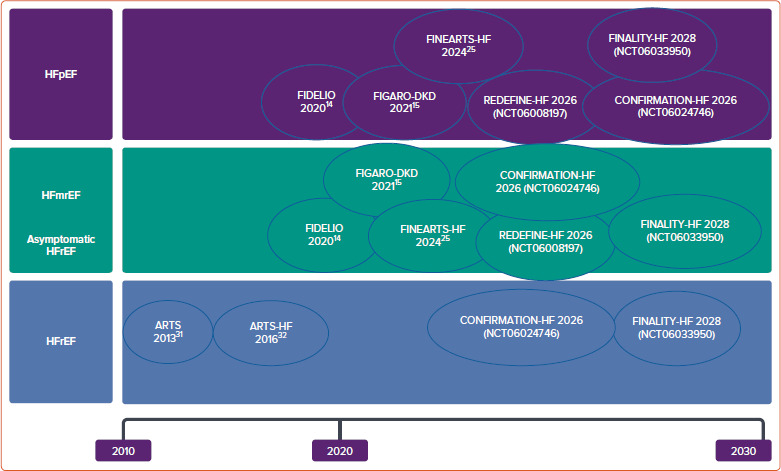
Heart failure (HF) is a major contributor to hospitalisations and accounts for 7% of cardiovascular-related deaths, with patients who have chronic kidney disease and type 2 diabetes at heightened risk. Existing treatment guidelines inadequately address these comorbidities. Steroidal mineralocorticoid receptor antagonists (MRAs) are commonly used in HF with reduced ejection fraction but pose risks, such as hyperkalaemia and acute kidney injury. Finerenone, a non-steroidal MRA, offers a safer alternative, with higher selectivity, reduced electrolyte disturbances and beneficial effects on heart and kidney tissues. Preclinical studies show anti-inflammatory and anti-fibrotic effects, while phase III trials (ARTS and ARTS-HF) demonstrated fewer hyperkalaemia incidents compared with spironolactone. In phase III trials (FIDELIO-DKD and FIGARO-DKD), finerenone reduced HF hospitalisations by 22% in patients with chronic kidney disease and type 2 diabetes. The FINEARTS-HF trial found that finerenone significantly reduced the risk of worsening HF events or CV death in patients with HF with mildly reduced or preserved ejection fraction. Its combination with therapies, such as sodium-glucose cotransporter 2 inhibitors, shows promise and ongoing trials, such as REDEFINE-HF, FINALITY-HF and CONFIRMATION-HF, are investigating its efficacy in other HF phenotypes. These studies will further establish the role of finerenone in managing cardio-renal-metabolic diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


