Polymicrobial infection presenting as non-clostridial gas gangrene in a patient with an open pelvic ring fracture accompanied by abdominal evisceration: a case report.
{"title":"Polymicrobial infection presenting as non-clostridial gas gangrene in a patient with an open pelvic ring fracture accompanied by abdominal evisceration: a case report.","authors":"Kenichi Takeno, Motoki Sugano, Yasuo Kokubo","doi":"10.21037/acr-24-128","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Open pelvic fractures are rare but represent a serious clinical problem with high mortality rates. Acute mortality is often associated with hemorrhage, whereas delayed mortality is most often associated with sepsis and multiple organ failure. We report a case of Wang's classification of type II open pelvic ring fracture with hemorrhagic shock and septic shock from gas gangrene.</p><p><strong>Case description: </strong>A healthy 41-year-old man presented with an open pelvic ring fracture and a laceration in the lower abdomen sustained at an ironworks. His hemodynamic status was unstable. Pelvic ring stabilization with an external fixator, ligation of the median sacral and bilateral internal iliac arteries, partial resection of the ileum, appendectomy, and intra-abdominal pelvic packing were performed. Seven days after the injury, he developed a single spike fever of 39.8 ℃ with a significant pus discharge from the open wound around his groin. A computed tomography scan revealed an accumulation of gas around the sacroiliac joint, in the abdominal cavity, and the adductors and gluteus maximus muscles caused by non-clostridial gas gangrene. We performed surgical debridement three times and initiated vancomycin administration. Hyperbaric oxygen therapy was also initiated as an adjunctive therapy. The patient could walk with a cane 5 months after the injury.</p><p><strong>Conclusions: </strong>We described a multidisciplinary case of a patient with a Wang type II open pelvic fracture who required emergent damage control and subsequently developed anaerobic sepsis. Bleeding was controlled by packing gauze into the intraperitoneal cavity and applying external fixation to the pelvic ring. However, it is important to administer prophylactic antibiotics against anaerobic bacteria and to detect subsequent infections early when packing gauze into the intraperitoneal cavity in patients with open pelvic fractures.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"29"},"PeriodicalIF":0.7000,"publicationDate":"2024-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11759928/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-128","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Open pelvic fractures are rare but represent a serious clinical problem with high mortality rates. Acute mortality is often associated with hemorrhage, whereas delayed mortality is most often associated with sepsis and multiple organ failure. We report a case of Wang's classification of type II open pelvic ring fracture with hemorrhagic shock and septic shock from gas gangrene.
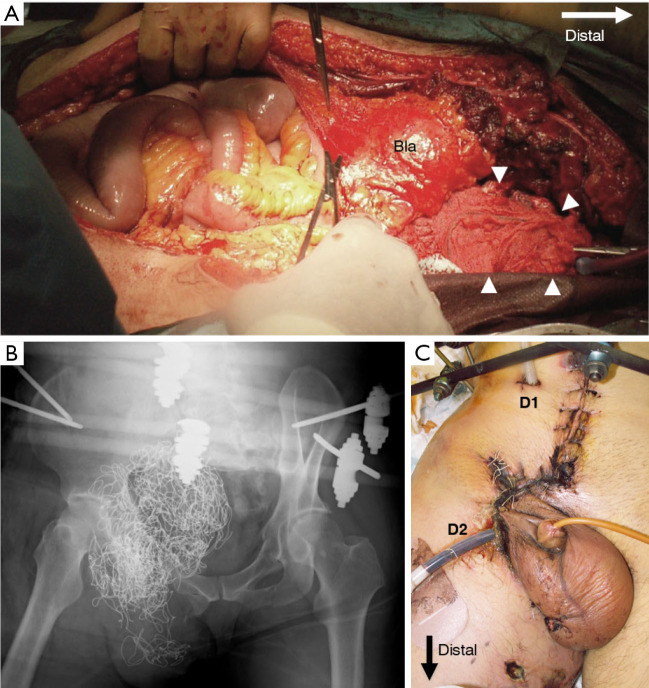
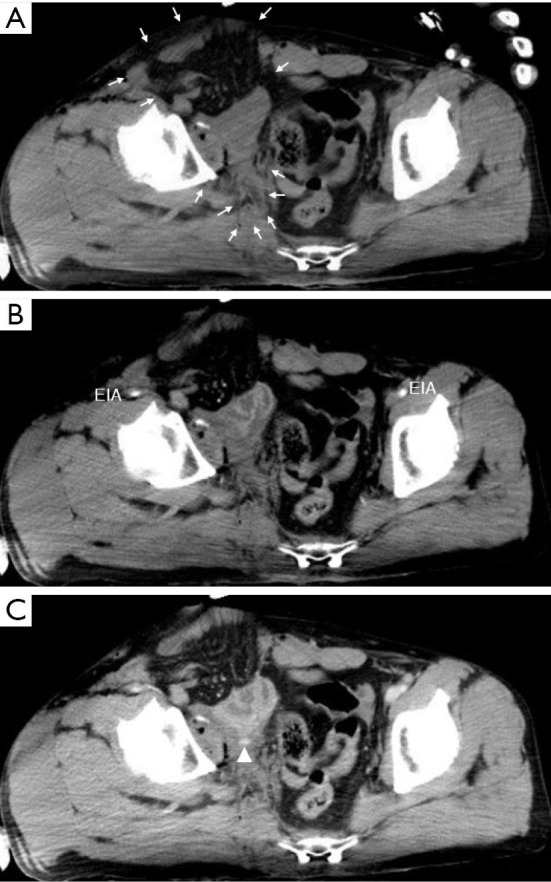
Case description: A healthy 41-year-old man presented with an open pelvic ring fracture and a laceration in the lower abdomen sustained at an ironworks. His hemodynamic status was unstable. Pelvic ring stabilization with an external fixator, ligation of the median sacral and bilateral internal iliac arteries, partial resection of the ileum, appendectomy, and intra-abdominal pelvic packing were performed. Seven days after the injury, he developed a single spike fever of 39.8 ℃ with a significant pus discharge from the open wound around his groin. A computed tomography scan revealed an accumulation of gas around the sacroiliac joint, in the abdominal cavity, and the adductors and gluteus maximus muscles caused by non-clostridial gas gangrene. We performed surgical debridement three times and initiated vancomycin administration. Hyperbaric oxygen therapy was also initiated as an adjunctive therapy. The patient could walk with a cane 5 months after the injury.
Conclusions: We described a multidisciplinary case of a patient with a Wang type II open pelvic fracture who required emergent damage control and subsequently developed anaerobic sepsis. Bleeding was controlled by packing gauze into the intraperitoneal cavity and applying external fixation to the pelvic ring. However, it is important to administer prophylactic antibiotics against anaerobic bacteria and to detect subsequent infections early when packing gauze into the intraperitoneal cavity in patients with open pelvic fractures.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


