Gabriel de Azambuja Beigin, Joao Henrique Godoy Rodrigues, Murillo de Souza Tuckumantel, Waldomiro Camargo, Ana Beatriz Souza de Oliveira, Abel Guilherme Rosa, Luis Cesar Fava Spessoto, Fernando Nestor Facio Júnior, Carlos Abib Cury
{"title":"Giant prostatic calculus in patient treated with perineal prostatotomy: case report.","authors":"Gabriel de Azambuja Beigin, Joao Henrique Godoy Rodrigues, Murillo de Souza Tuckumantel, Waldomiro Camargo, Ana Beatriz Souza de Oliveira, Abel Guilherme Rosa, Luis Cesar Fava Spessoto, Fernando Nestor Facio Júnior, Carlos Abib Cury","doi":"10.21037/acr-23-115","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Urolithiasis (kidney stone) is a common condition that often leads patients to urgent or emergency care services. Urinary calculi are generally found in the kidneys, ureters, or bladder. Urethral calculi are uncommon and can result from the migration of a calculus in the upper urinary tract or vesicle or may be primary of the urethra. Prostatic calculi are a rarity.</p><p><strong>Case description: </strong>A 34-year-old male was admitted to the emergency service of a university hospital reporting dysuria and pain in the hypogastrium with a 4-day history. The patient reported that the pain sometimes irradiated to the left flank, accompanied by micturition effort, a weak urinary stream, pollakiuria, and urine output with a crystal appearance. The clinical history revealed urinary difficulty since 10 years of age. The patient was submitted to radiological investigation. Pelvic computed tomography revealed a voluminous calculus with slightly lobulated contours in the intravesical topography in the interior of the prostatic urethra. Urethrocystography revealed a prostatic calculus and the tapered passage of contrast through the prostatic urethra. After the diagnosis, the rectal examination confirmed the presence of a hardened calculous mass in the prostatic topography. Considering the complementary evaluation of the patient, perineal prostatotomy was planned. Prostatotomy was performed longitudinally in the prostatic capsule for the removal of the calculus after its release by dissection.</p><p><strong>Conclusions: </strong>In cases of patients with urinary retention treated at an emergency service, the following diagnostic hypotheses should be investigated: benign hyperplasia of the prostate, urethral stenosis, prostatic urethral calculus, and prostatic calculus. In prostatic calculus, regarding access for definitive surgery, in this case, the perineal route proved to be the best therapeutic option.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"12"},"PeriodicalIF":0.7000,"publicationDate":"2024-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11760513/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-23-115","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Urolithiasis (kidney stone) is a common condition that often leads patients to urgent or emergency care services. Urinary calculi are generally found in the kidneys, ureters, or bladder. Urethral calculi are uncommon and can result from the migration of a calculus in the upper urinary tract or vesicle or may be primary of the urethra. Prostatic calculi are a rarity.
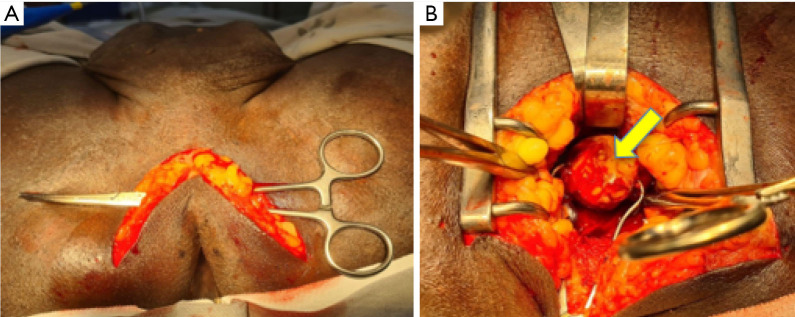
Case description: A 34-year-old male was admitted to the emergency service of a university hospital reporting dysuria and pain in the hypogastrium with a 4-day history. The patient reported that the pain sometimes irradiated to the left flank, accompanied by micturition effort, a weak urinary stream, pollakiuria, and urine output with a crystal appearance. The clinical history revealed urinary difficulty since 10 years of age. The patient was submitted to radiological investigation. Pelvic computed tomography revealed a voluminous calculus with slightly lobulated contours in the intravesical topography in the interior of the prostatic urethra. Urethrocystography revealed a prostatic calculus and the tapered passage of contrast through the prostatic urethra. After the diagnosis, the rectal examination confirmed the presence of a hardened calculous mass in the prostatic topography. Considering the complementary evaluation of the patient, perineal prostatotomy was planned. Prostatotomy was performed longitudinally in the prostatic capsule for the removal of the calculus after its release by dissection.
Conclusions: In cases of patients with urinary retention treated at an emergency service, the following diagnostic hypotheses should be investigated: benign hyperplasia of the prostate, urethral stenosis, prostatic urethral calculus, and prostatic calculus. In prostatic calculus, regarding access for definitive surgery, in this case, the perineal route proved to be the best therapeutic option.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


