Ennio Polilli, Paola Volpe, Jessica Elisabetta Esposito, Annalisa Di Risio, Caterina Di Carmine, Giancarlo Di Iorio, Marco Gabini, Pierluigi Tocco
{"title":"AQP4 antibody-seropositive neuromyelitis optica spectrum disorder in a patient with mixed connective tissue disease: a case report.","authors":"Ennio Polilli, Paola Volpe, Jessica Elisabetta Esposito, Annalisa Di Risio, Caterina Di Carmine, Giancarlo Di Iorio, Marco Gabini, Pierluigi Tocco","doi":"10.21037/acr-23-48","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neuromyelitis optica spectrum disorders (NMOSDs) are degenerative diseases frequently associated with severe recurrences and high risk of progressive disability. In this report, we describe an unusual case of a patient with the coexistence between NMOSD and mixed connective tissue disease (MCTD).</p><p><strong>Case description: </strong>A 58-year-old Caucasian man was admitted to the Emergency Department (ED) with low back pain and walking inability. He had an unsteady gait, paraesthesia of the lower limbs and pain in the left lumbar area of the spine. He previously manifested repeated episodes of Raynaud's phenomenon. The neurological examination revealed pyramidal signs with asymmetric and progressive paraparesis associated with hypoesthesia and bladder dysfunction. A spine magnetic resonance imaging (MRI) revealed the presence of a long extensive cervico-dorsal myelitis. Among laboratory analyses, serum immunometric examinations came back positive for anti-RNP (272 U/mL) and anti-SSA (20 U/mL) antibodies, whereas a recombinant immunofluorescence assay revealed the presence of immunoglobulin G (IgG) antibodies against AQP4. Consequently, he was treated with high-doses of corticosteroids, with progressive resolution of symptoms. To date, his last cervico-dorsal spine MRI showed negative results.</p><p><strong>Conclusions: </strong>Only a few anecdotal cases of the coexistence between NMOSD and MCTD have so far been described, and many clinical aspects of this association are not yet fully known. Missed diagnosis of rheumatologic or neurologic diseases may lead to treatment delay and, potentially, irreversible disability. Closer collaboration between neurologists and rheumatologists is needed for the early diagnosis of both diseases.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"30"},"PeriodicalIF":0.7000,"publicationDate":"2024-12-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11761318/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-23-48","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Neuromyelitis optica spectrum disorders (NMOSDs) are degenerative diseases frequently associated with severe recurrences and high risk of progressive disability. In this report, we describe an unusual case of a patient with the coexistence between NMOSD and mixed connective tissue disease (MCTD).
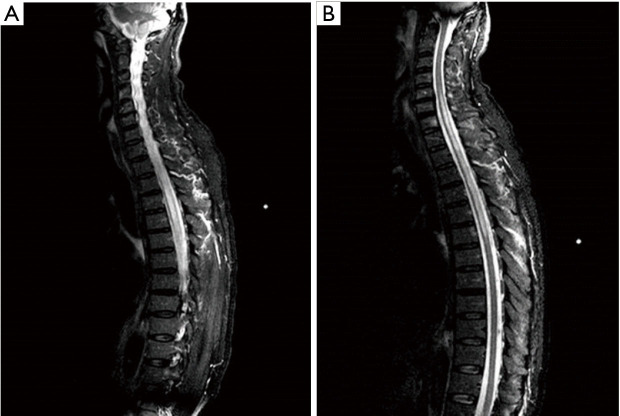
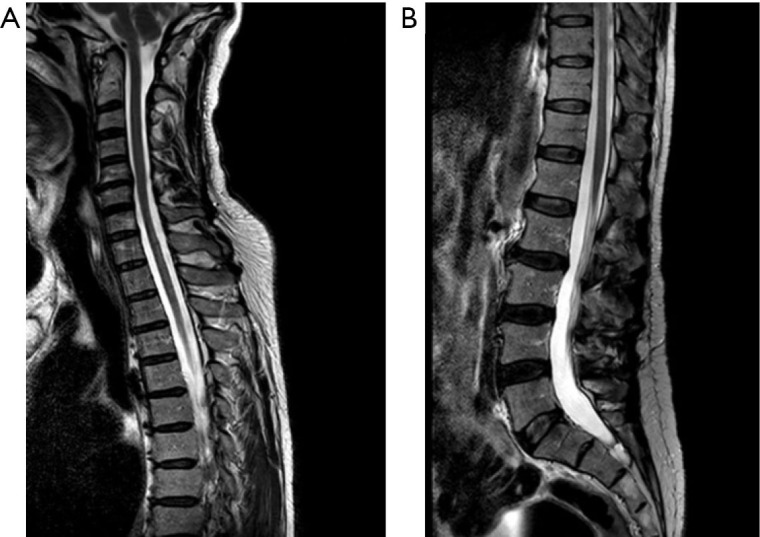
Case description: A 58-year-old Caucasian man was admitted to the Emergency Department (ED) with low back pain and walking inability. He had an unsteady gait, paraesthesia of the lower limbs and pain in the left lumbar area of the spine. He previously manifested repeated episodes of Raynaud's phenomenon. The neurological examination revealed pyramidal signs with asymmetric and progressive paraparesis associated with hypoesthesia and bladder dysfunction. A spine magnetic resonance imaging (MRI) revealed the presence of a long extensive cervico-dorsal myelitis. Among laboratory analyses, serum immunometric examinations came back positive for anti-RNP (272 U/mL) and anti-SSA (20 U/mL) antibodies, whereas a recombinant immunofluorescence assay revealed the presence of immunoglobulin G (IgG) antibodies against AQP4. Consequently, he was treated with high-doses of corticosteroids, with progressive resolution of symptoms. To date, his last cervico-dorsal spine MRI showed negative results.
Conclusions: Only a few anecdotal cases of the coexistence between NMOSD and MCTD have so far been described, and many clinical aspects of this association are not yet fully known. Missed diagnosis of rheumatologic or neurologic diseases may lead to treatment delay and, potentially, irreversible disability. Closer collaboration between neurologists and rheumatologists is needed for the early diagnosis of both diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


