{"title":"Uterine cystic adenomyosis: a case report.","authors":"Xudong Ma, Jinlu Shen, Rongrong Tang, Fangying Sun, Wenjie Chen, Jianhua Yang","doi":"10.21037/acr-24-143","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Uterine cystic adenomyosis (CA) is a unique form of adenomyosis with a single or fused lumen of the cystic space exceeding a diameter of 1 cm that typically results in progressively worsening dysmenorrhea. In most cases, the prognosis and pregnancy outcomes of CA remained unclear, and therefore further studies are warranted.</p><p><strong>Case description: </strong>A 19‑year‑old woman was admitted for irregular vaginal bleeding that lasted for more than one month. Transabdominal B-ultrasound examination revealed a hypoechoic nodule measuring approximately 4.8 cm × 3.9 cm × 4.9 cm that is situated on the posterior wall of the uterus, in close proximity to the uterine fundus. The preoperative diagnosis was concluded as a pelvic mass with a cancer antigen 125 (CA125) level of 51.48 U/mL. She accepted a laparoscopic myomectomy and the CA lesion crossing the myometrium was removed. During operation, dense adhesions were found among a portion of the colorectum, omentum, uterus and bilateral adnexal areas. A cystic mass of approximately 7.0 cm × 5.0 cm × 4.0 cm was visible in the posterior wall of the uterus, and a sinus of approximately 1.0 cm in diameter was found to be connected to the uterine cavity at the lower posterior wall of the uterus, and the cystic wall was attached to the endometrium. Based on the classification criteria of MUSCLE (myometrial location, uterine site, structure, contents, level, endometrial or inner lining), the current case is classified as an A1-B1 mixed type. Following surgery, GnRH-a consolidation therapy was applied for 3 months. Such treatment relieved her symptoms and improved her quality of life while preserving her reproductive function.</p><p><strong>Conclusions: </strong>This is the first reported case of an A1-B1 mixed type CA that was successfully treated by laparoscopic surgery supplemented with GnRH-a consolidation therapy.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"23"},"PeriodicalIF":0.7000,"publicationDate":"2024-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11760926/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-143","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Uterine cystic adenomyosis (CA) is a unique form of adenomyosis with a single or fused lumen of the cystic space exceeding a diameter of 1 cm that typically results in progressively worsening dysmenorrhea. In most cases, the prognosis and pregnancy outcomes of CA remained unclear, and therefore further studies are warranted.
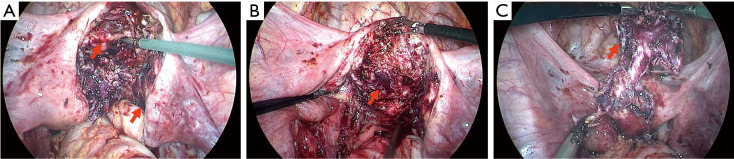
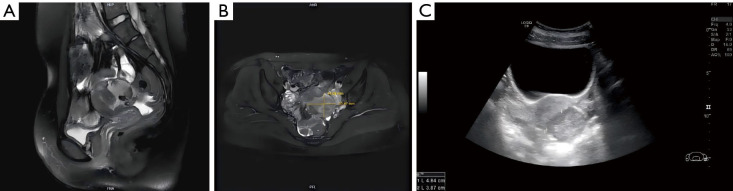
Case description: A 19‑year‑old woman was admitted for irregular vaginal bleeding that lasted for more than one month. Transabdominal B-ultrasound examination revealed a hypoechoic nodule measuring approximately 4.8 cm × 3.9 cm × 4.9 cm that is situated on the posterior wall of the uterus, in close proximity to the uterine fundus. The preoperative diagnosis was concluded as a pelvic mass with a cancer antigen 125 (CA125) level of 51.48 U/mL. She accepted a laparoscopic myomectomy and the CA lesion crossing the myometrium was removed. During operation, dense adhesions were found among a portion of the colorectum, omentum, uterus and bilateral adnexal areas. A cystic mass of approximately 7.0 cm × 5.0 cm × 4.0 cm was visible in the posterior wall of the uterus, and a sinus of approximately 1.0 cm in diameter was found to be connected to the uterine cavity at the lower posterior wall of the uterus, and the cystic wall was attached to the endometrium. Based on the classification criteria of MUSCLE (myometrial location, uterine site, structure, contents, level, endometrial or inner lining), the current case is classified as an A1-B1 mixed type. Following surgery, GnRH-a consolidation therapy was applied for 3 months. Such treatment relieved her symptoms and improved her quality of life while preserving her reproductive function.
Conclusions: This is the first reported case of an A1-B1 mixed type CA that was successfully treated by laparoscopic surgery supplemented with GnRH-a consolidation therapy.
背景:子宫囊性血凝块(CA)是一种独特形式的血凝块,囊腔的单个或融合腔直径超过1cm,通常导致痛经逐渐加重。在大多数情况下,CA的预后和妊娠结局仍不清楚,因此需要进一步的研究。病例描述:一名19岁女性因持续一个多月的不规则阴道出血入院。经腹b超检查发现子宫后壁约4.8 cm × 3.9 cm × 4.9 cm的低回声结节,靠近子宫底。术前诊断为盆腔肿块,癌抗原125 (CA125)水平51.48 U/mL。她接受了腹腔镜子宫肌瘤切除术,跨越子宫内膜的CA病变被切除。术中发现结直肠、大网膜、子宫及双侧附件部分粘连。子宫后壁可见一个约7.0 cm × 5.0 cm × 4.0 cm的囊性肿块,在子宫后壁下方发现一个直径约1.0 cm的窦腔与子宫腔相连,囊壁附着于子宫内膜。根据肌的分类标准(子宫肌层位置、子宫部位、结构、内容物、水平、子宫内膜或内膜),本例为A1-B1混合型。术后给予GnRH-a巩固治疗3个月。这种治疗缓解了她的症状,改善了她的生活质量,同时保留了她的生殖功能。结论:这是首例经腹腔镜手术配合GnRH-a巩固治疗成功的A1-B1混合型CA病例。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


