Hua Xie, Xiaojun Zhang, Junli Zhang, Meicen Liu, Xiangqian Che
{"title":"The diagnosis of eosinophilic granulomatosis with polyangiitis has been 'masked' by asthma: a case report.","authors":"Hua Xie, Xiaojun Zhang, Junli Zhang, Meicen Liu, Xiangqian Che","doi":"10.21037/acr-24-79","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with asthma exhibit a significantly heightened susceptibility to eosinophilic granulomatosis with polyangiitis (EGPA) when compared to the general population. Vigilance for EGPA manifestations is crucial, especially in cases where asthma remains poorly controlled despite high-dose corticosteroid therapy or when eosinophil counts exceed 5%. The diagnosis of EGPA can be complex due to the absence of definitive biomarkers, as indicated by the American College of Rheumatology (ACR)'s 1990 classification criteria. EGPA is categorized as an antineutrophil cytoplasmic antibody (ANCA) associated vasculitis, with updated classification criteria released in 2022, which require a cumulative score of 6 or more for the diagnosis of small and medium vessel vasculitis. Enhancing knowledge of EGPA facilitates its early detection and effective management.</p><p><strong>Case description: </strong>The patient was initially diagnosed with allergic rhinitis in 2006 and developed cough and wheezing in 2016. In 2017, EGPA was diagnosed based on ACR criteria, with a cumulative score of 14 according to the 2022 ACR and the European League Against Rheumatism (ACR/EULAR) criteria, indicating small and medium vessel vasculitis. The patient showed myocardial, gastric, and neurological involvement, reflecting generalized EGPA. Prognostic assessments should use the five-factor score (FFS), which indicates a 46% 5-year mortality rate for those with an FFS of 2 or higher. This patient had an FFS of 3, tested negative for ANCA, and cardiac emission computed tomography (ECT) confirmed myocardial involvement. However, as EGPA was diagnosed only 13 months after the onset of wheezing, the patient had been undergoing glucocorticoid therapy, as of today (7 years later), has effectively managed the symptoms and facilitated normal daily activities.</p><p><strong>Conclusions: </strong>If asthma symptoms persist despite intensive corticosteroid treatment or the eosinophil count exceeds 5%, consider the possibility of EGPA. The presence of ANCA exerts a substantial impact on the prognostic outcomes in EGPA. ANCA-negative patients typically exhibit reduced survival rates, primarily attributed to a higher incidence of cardiac involvement. Nevertheless, advancements in early diagnosis and therapeutic interventions have led to improved survival rates, even in cases complicated by cardiac and pulmonary manifestations.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"31"},"PeriodicalIF":0.7000,"publicationDate":"2024-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11760517/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-79","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with asthma exhibit a significantly heightened susceptibility to eosinophilic granulomatosis with polyangiitis (EGPA) when compared to the general population. Vigilance for EGPA manifestations is crucial, especially in cases where asthma remains poorly controlled despite high-dose corticosteroid therapy or when eosinophil counts exceed 5%. The diagnosis of EGPA can be complex due to the absence of definitive biomarkers, as indicated by the American College of Rheumatology (ACR)'s 1990 classification criteria. EGPA is categorized as an antineutrophil cytoplasmic antibody (ANCA) associated vasculitis, with updated classification criteria released in 2022, which require a cumulative score of 6 or more for the diagnosis of small and medium vessel vasculitis. Enhancing knowledge of EGPA facilitates its early detection and effective management.
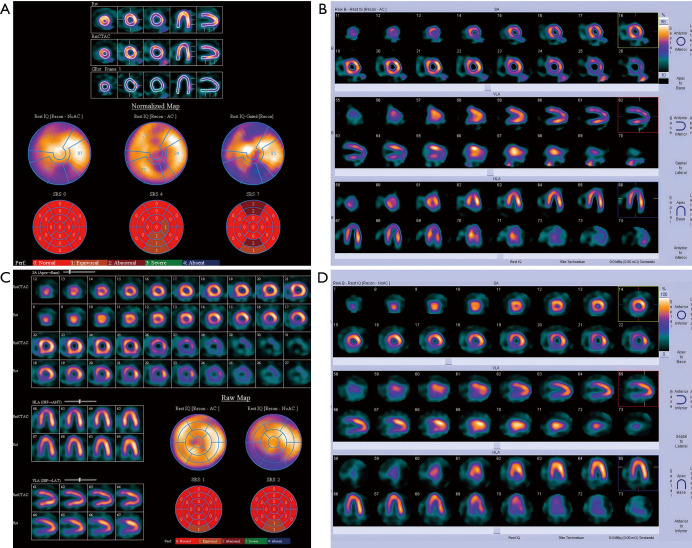
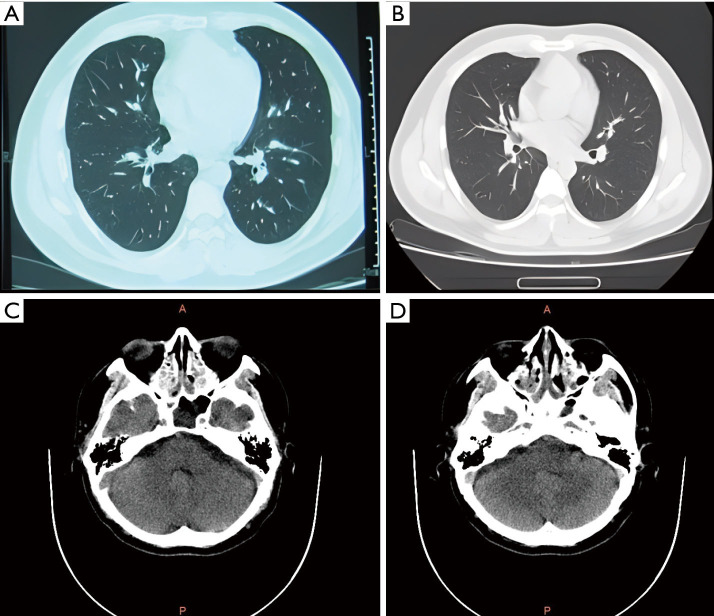
Case description: The patient was initially diagnosed with allergic rhinitis in 2006 and developed cough and wheezing in 2016. In 2017, EGPA was diagnosed based on ACR criteria, with a cumulative score of 14 according to the 2022 ACR and the European League Against Rheumatism (ACR/EULAR) criteria, indicating small and medium vessel vasculitis. The patient showed myocardial, gastric, and neurological involvement, reflecting generalized EGPA. Prognostic assessments should use the five-factor score (FFS), which indicates a 46% 5-year mortality rate for those with an FFS of 2 or higher. This patient had an FFS of 3, tested negative for ANCA, and cardiac emission computed tomography (ECT) confirmed myocardial involvement. However, as EGPA was diagnosed only 13 months after the onset of wheezing, the patient had been undergoing glucocorticoid therapy, as of today (7 years later), has effectively managed the symptoms and facilitated normal daily activities.
Conclusions: If asthma symptoms persist despite intensive corticosteroid treatment or the eosinophil count exceeds 5%, consider the possibility of EGPA. The presence of ANCA exerts a substantial impact on the prognostic outcomes in EGPA. ANCA-negative patients typically exhibit reduced survival rates, primarily attributed to a higher incidence of cardiac involvement. Nevertheless, advancements in early diagnosis and therapeutic interventions have led to improved survival rates, even in cases complicated by cardiac and pulmonary manifestations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


