{"title":"High Middle Cerebral Artery Wall Shear Stress in Branch Atheromatous Disease: A Computational Fluid Dynamics Analysis.","authors":"Yorito Hattori, Shuta Imada, Ryo Usui, Akimasa Yamamoto, Masanori Nakamura, Masafumi Ihara","doi":"10.5551/jat.65439","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>Branch atheromatous disease (BAD), characterized by the occlusion of perforating branches near the orifice of a parent artery, often develops early neurological deterioration because the mechanisms underlying BAD remain unclear. Abnormal wall shear stress (WSS) is strongly associated with endothelial dysfunction and plaque growth or rupture. Therefore, we hypothesized that computational fluid dynamics (CFD) modeling could detect differences in WSS between BAD and small-vessel occlusion (SVO), both of which result from perforating artery occlusion/stenosis.</p><p><strong>Methods: </strong>This cross-sectional observational study included consecutive patients admitted to our institution within 7 days after symptom onset who met the following criteria: absence of stenosis/occlusion in the intracranial major arteries on brain magnetic resonance angiography (MRA) or extracranial carotid arteries on carotid ultrasonography. The WSS and blood flow velocity in the M1 segment of the middle cerebral artery were analyzed using CFD based on MRA.</p><p><strong>Results: </strong>The number of patients with a WSS ratio (ipsilesional/contralesional) of >1 was significantly higher in patients with BAD (n = 27) than in those with SVO (n = 27) [20 (74.1%) vs. 11 (40.7%), p = 0.013]. Higher WSS on ipsilesional M1 than on contralesional M1 was an independent risk factor for BAD (adjusted odds ratio 4.38, 95% confidence interval 1.29-14.82, p = 0.018). Blood flow velocity in the M1 segment was not associated with BAD.</p><p><strong>Conclusions: </strong>In patients with BAD, higher M1 segment WSS on CFD can be a risk factor for the development of vulnerable plaques in branch orifices. Moreover, the use of CFD may contribute to the diagnosis of BAD.</p>","PeriodicalId":15128,"journal":{"name":"Journal of atherosclerosis and thrombosis","volume":" ","pages":"994-1005"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12328737/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of atherosclerosis and thrombosis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5551/jat.65439","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: Branch atheromatous disease (BAD), characterized by the occlusion of perforating branches near the orifice of a parent artery, often develops early neurological deterioration because the mechanisms underlying BAD remain unclear. Abnormal wall shear stress (WSS) is strongly associated with endothelial dysfunction and plaque growth or rupture. Therefore, we hypothesized that computational fluid dynamics (CFD) modeling could detect differences in WSS between BAD and small-vessel occlusion (SVO), both of which result from perforating artery occlusion/stenosis.
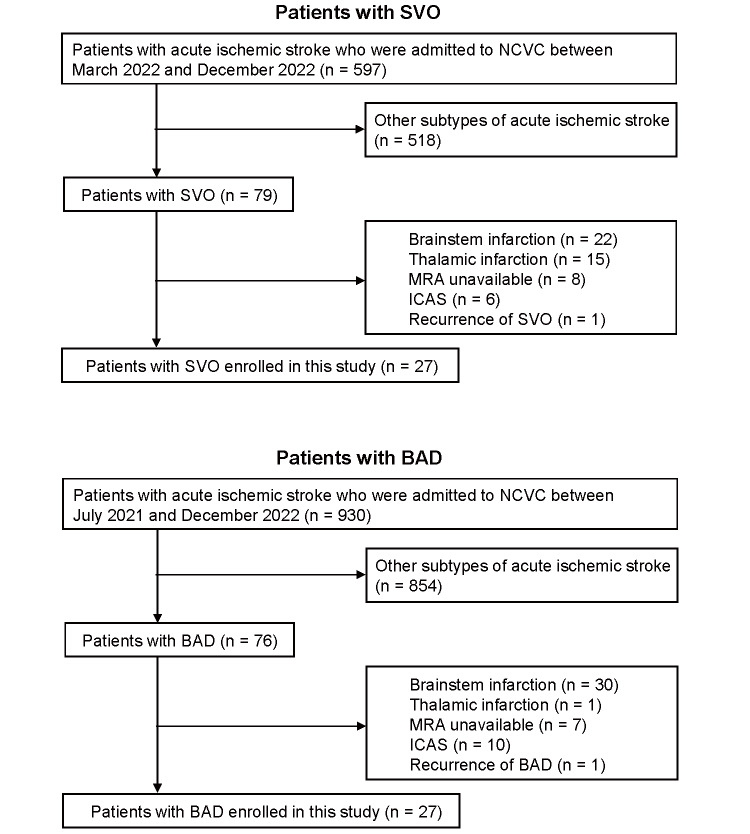
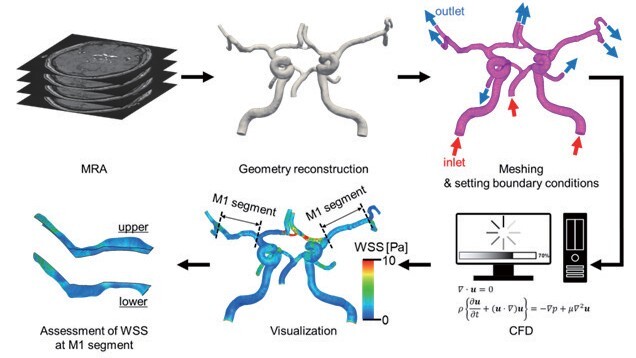
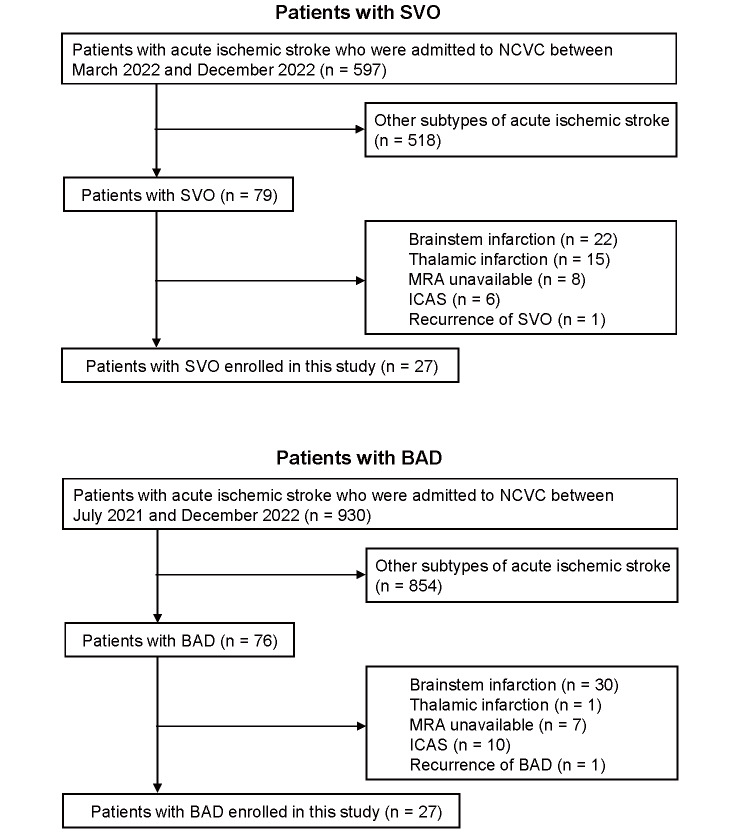
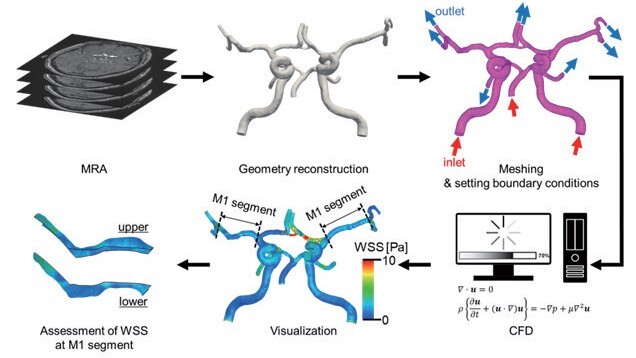
Methods: This cross-sectional observational study included consecutive patients admitted to our institution within 7 days after symptom onset who met the following criteria: absence of stenosis/occlusion in the intracranial major arteries on brain magnetic resonance angiography (MRA) or extracranial carotid arteries on carotid ultrasonography. The WSS and blood flow velocity in the M1 segment of the middle cerebral artery were analyzed using CFD based on MRA.
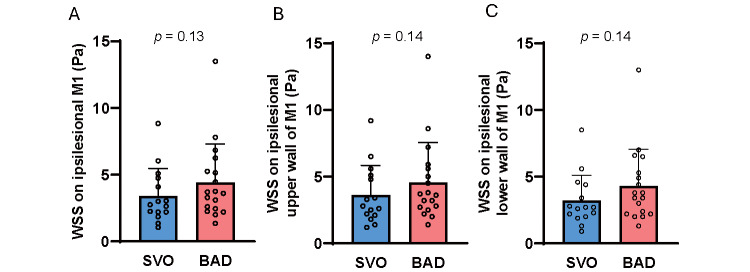
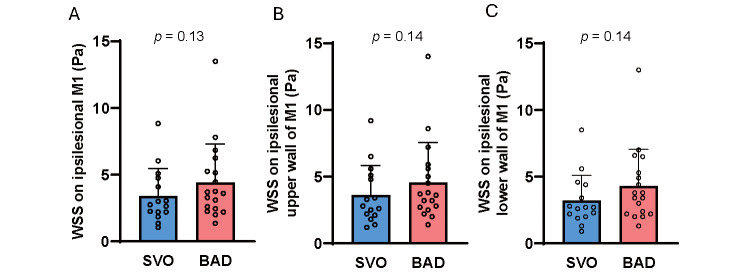
Results: The number of patients with a WSS ratio (ipsilesional/contralesional) of >1 was significantly higher in patients with BAD (n = 27) than in those with SVO (n = 27) [20 (74.1%) vs. 11 (40.7%), p = 0.013]. Higher WSS on ipsilesional M1 than on contralesional M1 was an independent risk factor for BAD (adjusted odds ratio 4.38, 95% confidence interval 1.29-14.82, p = 0.018). Blood flow velocity in the M1 segment was not associated with BAD.
Conclusions: In patients with BAD, higher M1 segment WSS on CFD can be a risk factor for the development of vulnerable plaques in branch orifices. Moreover, the use of CFD may contribute to the diagnosis of BAD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


