Jordan Talan, Keshav Mangalick, Deepak Pradhan, Harald Sauthoff
{"title":"Accuracy of Echocardiographic Cardiac Output Assessment by Critical Care Fellows.","authors":"Jordan Talan, Keshav Mangalick, Deepak Pradhan, Harald Sauthoff","doi":"10.34197/ats-scholar.2024-0030OC","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Advanced critical care echocardiography comprises a specific set of qualitative and quantitative point-of-care echocardiography skills, including a reliable, noninvasive method to measure cardiac output. This technique requires echocardiographic measurement of left ventricular outflow tract (LVOT) diameter and LVOT velocity time integral (VTI). Although there is a demand among critical care fellows to learn these advanced techniques, there are no data describing the acquisition of mastery in these skills.</p><p><strong>Objective: </strong>This pilot study aims to describe the accuracy of echocardiographic measurement of LVOT diameter and LVOT VTI obtained by critical care fellows after an educational intervention, as well as to enhance validation evidence for an image scoring assessment that is applicable to these measurements.</p><p><strong>Methods: </strong>We implemented a brief mastery learning intervention to teach the measurement of LVOT diameter and VTI. Fellow measurements of these parameters, along with the corresponding echocardiographic images, were compared with a gold standard of measurements obtained by professional echocardiography technicians and interpreted by cardiologists.</p><p><strong>Results: </strong>Seven fellows performed 35 echocardiograms on 32 patients. The average fellow-reported LVOT VTI was 17.0 ± 4.37 cm, whereas the average cardiologist-reported VTI was 17.3 ± 5.19 cm. The correlation (<i>r</i>) between fellow and cardiologist-reported VTI was 0.73 (<i>P</i> < 0.001), with a mean percent difference of 19.5 ± 12.0%. The average fellow-reported LVOT diameter was 2.07 ± 0.23 cm, whereas the average cardiologist-reported LVOT diameter was 2.08 ± 0.22 cm. The correlation (<i>r</i>) between fellow and cardiologist-reported LVOT diameter was 0.51 (<i>P</i> = 0.004), with a mean percent difference of 8.05 ± 7.0%. The sensitivity for fellows to detect an abnormal LVOT VTI was 91%, with a specificity of 43%.</p><p><strong>Conclusion: </strong>Critical care fellow measurement of LVOT VTI and LVOT diameter demonstrated strong and moderate positive correlations with cardiologist-reported values, respectively, with acceptable clinical agreement. However, interrater reliability and percent differences showed room for improvement. Education in these advanced skills is resource intensive, and additional research is needed to determine the most effective approach to training fellows.</p>","PeriodicalId":72330,"journal":{"name":"ATS scholar","volume":"5 4","pages":"547-558"},"PeriodicalIF":1.9000,"publicationDate":"2024-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11734671/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ATS scholar","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34197/ats-scholar.2024-0030OC","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Advanced critical care echocardiography comprises a specific set of qualitative and quantitative point-of-care echocardiography skills, including a reliable, noninvasive method to measure cardiac output. This technique requires echocardiographic measurement of left ventricular outflow tract (LVOT) diameter and LVOT velocity time integral (VTI). Although there is a demand among critical care fellows to learn these advanced techniques, there are no data describing the acquisition of mastery in these skills.
Objective: This pilot study aims to describe the accuracy of echocardiographic measurement of LVOT diameter and LVOT VTI obtained by critical care fellows after an educational intervention, as well as to enhance validation evidence for an image scoring assessment that is applicable to these measurements.
Methods: We implemented a brief mastery learning intervention to teach the measurement of LVOT diameter and VTI. Fellow measurements of these parameters, along with the corresponding echocardiographic images, were compared with a gold standard of measurements obtained by professional echocardiography technicians and interpreted by cardiologists.
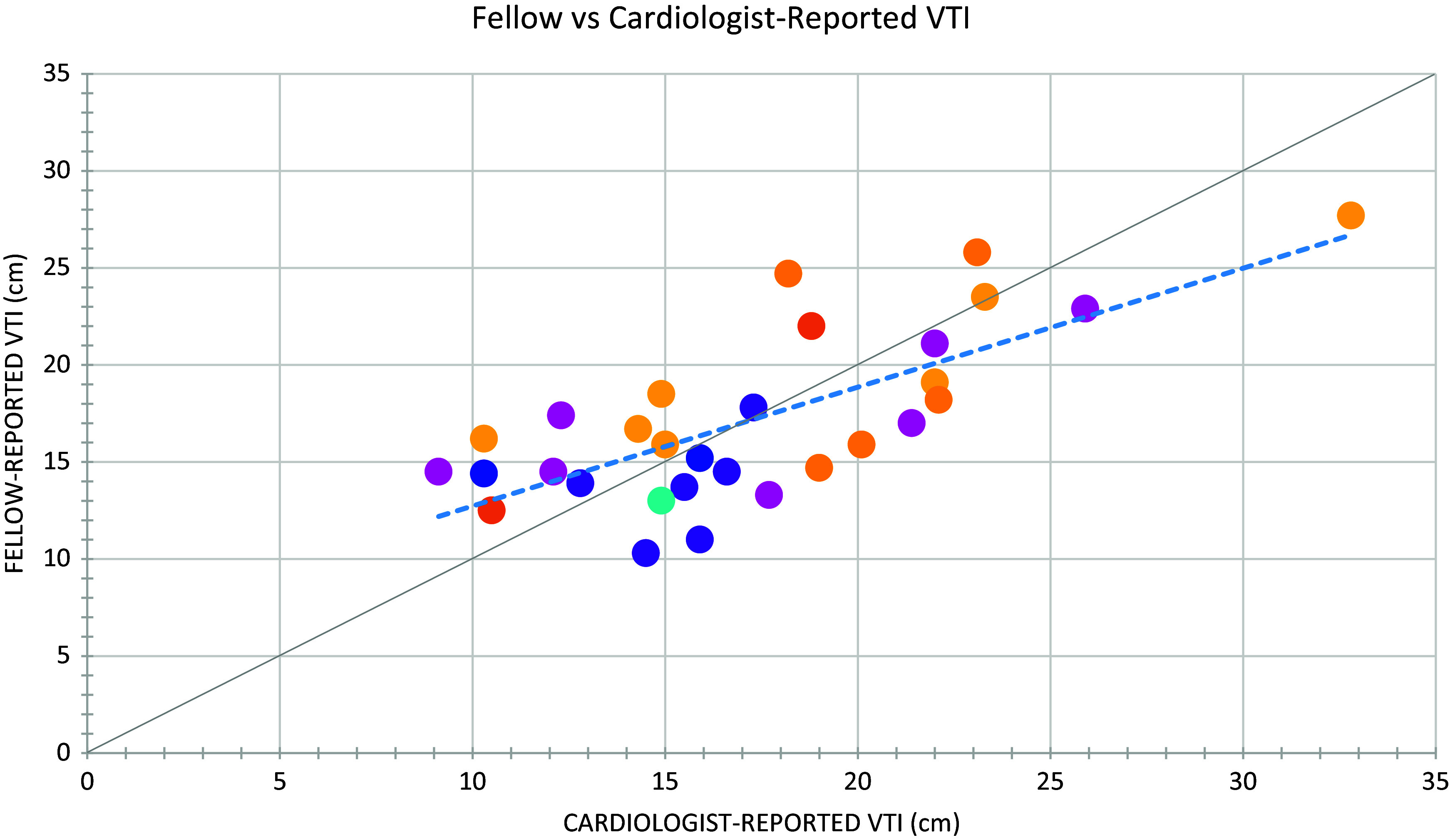
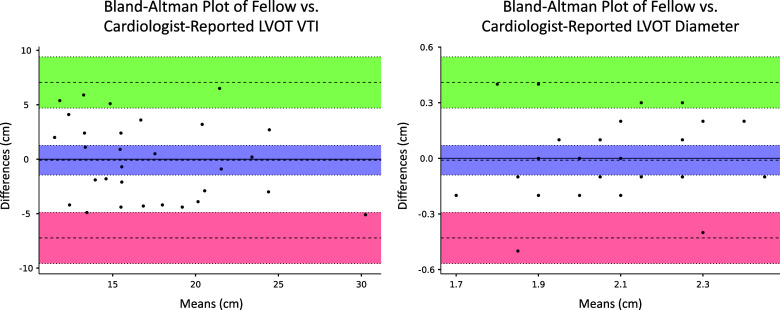
Results: Seven fellows performed 35 echocardiograms on 32 patients. The average fellow-reported LVOT VTI was 17.0 ± 4.37 cm, whereas the average cardiologist-reported VTI was 17.3 ± 5.19 cm. The correlation (r) between fellow and cardiologist-reported VTI was 0.73 (P < 0.001), with a mean percent difference of 19.5 ± 12.0%. The average fellow-reported LVOT diameter was 2.07 ± 0.23 cm, whereas the average cardiologist-reported LVOT diameter was 2.08 ± 0.22 cm. The correlation (r) between fellow and cardiologist-reported LVOT diameter was 0.51 (P = 0.004), with a mean percent difference of 8.05 ± 7.0%. The sensitivity for fellows to detect an abnormal LVOT VTI was 91%, with a specificity of 43%.
Conclusion: Critical care fellow measurement of LVOT VTI and LVOT diameter demonstrated strong and moderate positive correlations with cardiologist-reported values, respectively, with acceptable clinical agreement. However, interrater reliability and percent differences showed room for improvement. Education in these advanced skills is resource intensive, and additional research is needed to determine the most effective approach to training fellows.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


