Hyeung-Min Park, Jaram Lee, Soo Young Lee, Suk Hee Heo, Yong Yeon Jeong, Hyeong Rok Kim, Chang Hyun Kim
{"title":"Optimal extent of lymph node dissection in clinical early-stage right colon cancer: a retrospective analysis.","authors":"Hyeung-Min Park, Jaram Lee, Soo Young Lee, Suk Hee Heo, Yong Yeon Jeong, Hyeong Rok Kim, Chang Hyun Kim","doi":"10.4174/astr.2025.108.1.49","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Determining the extent of radical lymphadenectomy at clinical early stage is challenging. We aimed to investigate the appropriate extent of lymphadenectomy in clinical early-stage right colon cancer.</p><p><strong>Methods: </strong>Patients with clinical stage 0 or I right colon cancer who underwent curative surgery from January 2007 to December 2021 were included in this retrospective study. The extent of lymph node (LN) metastases based on the distribution of LN metastases (LND: LND1 pericolic nodes, LND2 intermediate nodes, LND3 apical nodes), along with the depth of submucosal (SM) invasion (classed into SM1-3), were analyzed.</p><p><strong>Results: </strong>Of the 348 patients, distribution across pathologic stages was as follows: 30 patients (8.6%) at stage 0, 207 (59.5%) at stage I, 52 (14.9%) at stage II, and 59 (17.0%) at stage III. In pT1 tumor patients, LN metastases varied by SM invasion depth: 3.6% in SM1 (all LND1), 5.1% in SM2 (all LND1), and 17.5% in SM3 (LND1 10%, LND2 5%, LND3 2.5%). For pT2, pT3, and pT4 stages, LN metastasis rates were 16.2% (LND1 11.3%, LND2 3.8%, LND3 1.3%), 39.7% (LND1 28.9%, LND2 8.4%, LND3 2.4%), and 50% (LND1 25%, LND2 25%), respectively. Tumor invasion depth and lymphovascular invasion were identified as significant risk factors for LN metastasis extending to LND2-3.</p><p><strong>Conclusion: </strong>Complete mesocolic excision should be considered for right-sided colon cancer because tumor infiltration deeper than SM2 could metastasize to LND2 or further. If preoperative endoscopy confirms SM1 or SM2 invasion, D2 lymphadenectomy could be a limited surgical option.</p>","PeriodicalId":8071,"journal":{"name":"Annals of Surgical Treatment and Research","volume":"108 1","pages":"49-56"},"PeriodicalIF":1.6000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11735168/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Surgical Treatment and Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4174/astr.2025.108.1.49","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Determining the extent of radical lymphadenectomy at clinical early stage is challenging. We aimed to investigate the appropriate extent of lymphadenectomy in clinical early-stage right colon cancer.
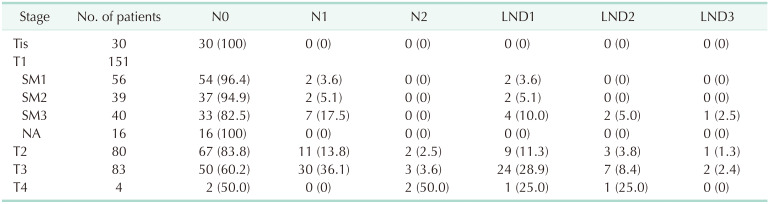
Methods: Patients with clinical stage 0 or I right colon cancer who underwent curative surgery from January 2007 to December 2021 were included in this retrospective study. The extent of lymph node (LN) metastases based on the distribution of LN metastases (LND: LND1 pericolic nodes, LND2 intermediate nodes, LND3 apical nodes), along with the depth of submucosal (SM) invasion (classed into SM1-3), were analyzed.
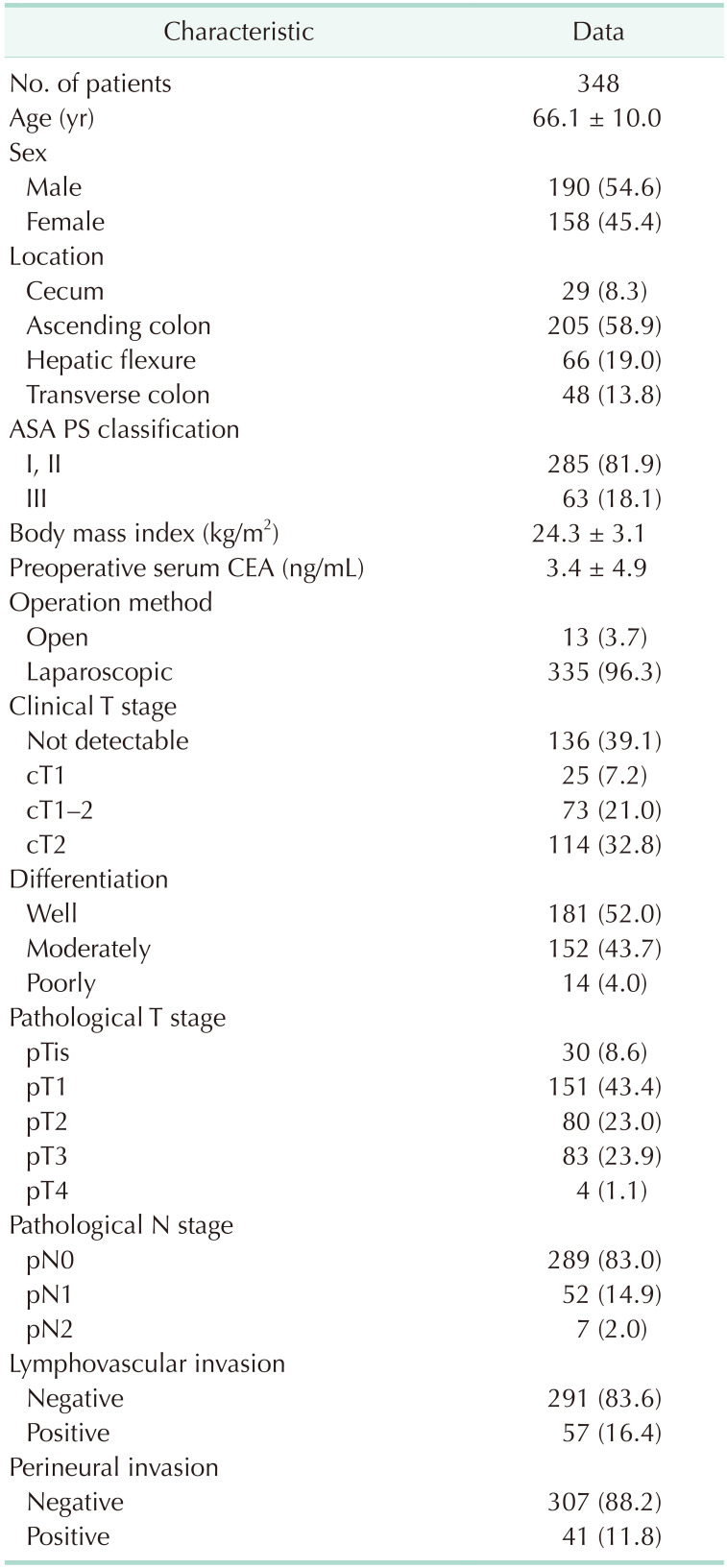
Results: Of the 348 patients, distribution across pathologic stages was as follows: 30 patients (8.6%) at stage 0, 207 (59.5%) at stage I, 52 (14.9%) at stage II, and 59 (17.0%) at stage III. In pT1 tumor patients, LN metastases varied by SM invasion depth: 3.6% in SM1 (all LND1), 5.1% in SM2 (all LND1), and 17.5% in SM3 (LND1 10%, LND2 5%, LND3 2.5%). For pT2, pT3, and pT4 stages, LN metastasis rates were 16.2% (LND1 11.3%, LND2 3.8%, LND3 1.3%), 39.7% (LND1 28.9%, LND2 8.4%, LND3 2.4%), and 50% (LND1 25%, LND2 25%), respectively. Tumor invasion depth and lymphovascular invasion were identified as significant risk factors for LN metastasis extending to LND2-3.
Conclusion: Complete mesocolic excision should be considered for right-sided colon cancer because tumor infiltration deeper than SM2 could metastasize to LND2 or further. If preoperative endoscopy confirms SM1 or SM2 invasion, D2 lymphadenectomy could be a limited surgical option.
期刊介绍:
Manuscripts to the Annals of Surgical Treatment and Research (Ann Surg Treat Res) should be written in English according to the instructions for authors. If the details are not described below, the style should follow the Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publications available at International Committee of Medical Journal Editors (ICMJE) website (http://www.icmje.org).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


