Is early use of sodium-glucose cotransporter type 2 inhibitor (SGLT2i) necessary even in diabetic patients without cardiovascular disease: a prospective study regarding the effect of SGLT2i on left ventricular diastolic function.
Kina Jeon, Shin Yi Jang, You-Bin Lee, Jihoon Kim, Darae Kim, Sung-A Chang, Sung-Ji Park, Sang-Chol Lee, Seung Woo Park, Moon-Kyu Lee, Eun Kyoung Kim, Kyu Yeon Hur
{"title":"Is early use of sodium-glucose cotransporter type 2 inhibitor (SGLT2i) necessary even in diabetic patients without cardiovascular disease: a prospective study regarding the effect of SGLT2i on left ventricular diastolic function.","authors":"Kina Jeon, Shin Yi Jang, You-Bin Lee, Jihoon Kim, Darae Kim, Sung-A Chang, Sung-Ji Park, Sang-Chol Lee, Seung Woo Park, Moon-Kyu Lee, Eun Kyoung Kim, Kyu Yeon Hur","doi":"10.1186/s44348-024-00043-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There are insufficient studies to determine whether sodium-glucose cotransporter type 2 inhibitors (SGLT2i) will help reduce early diabetic cardiomyopathy, especially in patients without documented cardiovascular disease.</p><p><strong>Methods: </strong>We performed a single center, prospective observation study. A total of 90 patients with type 2 diabetes patients without established heart failure or atherosclerotic cardiovascular disease were enrolled. Echocardiography, cardiac enzyme, and glucose-control data were examined before and 3 months after the administration of SGLT2i (dapagliflozin 10 mg per day). Cardiovascular risk factors included hypertension, smoking, obesity, dyslipidemia, and old age. The primary end point was the change of E/e' before and after administration of SGLT2i.</p><p><strong>Results: </strong>Most patients (86.7%) had three or more cardiovascular risk factors, and about 32% had all five risk factors. Although the decrease in E/e' after the administration of SGLT2i was observed in 20% of enrolled patients, there was no significant difference in average E/e' value or left atrial volume index before and after the SGLT2i medication. Even in patients with all known risk factors including old age, E/e' value did not decrease after adding SGLT2i (8.9 ± 2.4 vs. 8.7 ± 3.2). There was a statistically significant difference in E/e' change after the SGLT2i administration between patients younger than 60 years and those older than 60 years (-0.7 ± 2.2 vs. 1.1 ± 2.8, P = 0.002).</p><p><strong>Conclusions: </strong>In type 2 diabetes patients without documented cardiovascular disease including heart failure, administration of SGLT2i showed no improvement in diastolic function profile. Further large-scale randomized studies are needed to determine who will benefit from potential cardiovascular events with early addition of SGLT2i.</p>","PeriodicalId":15229,"journal":{"name":"Journal of Cardiovascular Imaging","volume":"33 1","pages":"1"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11727183/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Imaging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44348-024-00043-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There are insufficient studies to determine whether sodium-glucose cotransporter type 2 inhibitors (SGLT2i) will help reduce early diabetic cardiomyopathy, especially in patients without documented cardiovascular disease.
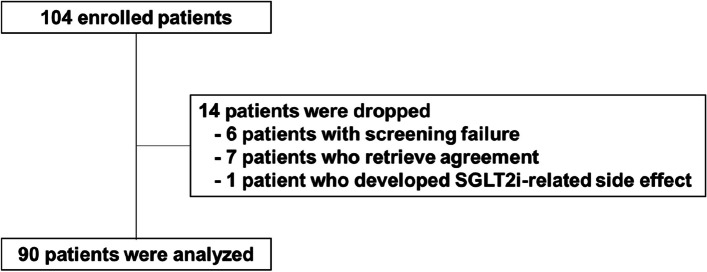
Methods: We performed a single center, prospective observation study. A total of 90 patients with type 2 diabetes patients without established heart failure or atherosclerotic cardiovascular disease were enrolled. Echocardiography, cardiac enzyme, and glucose-control data were examined before and 3 months after the administration of SGLT2i (dapagliflozin 10 mg per day). Cardiovascular risk factors included hypertension, smoking, obesity, dyslipidemia, and old age. The primary end point was the change of E/e' before and after administration of SGLT2i.
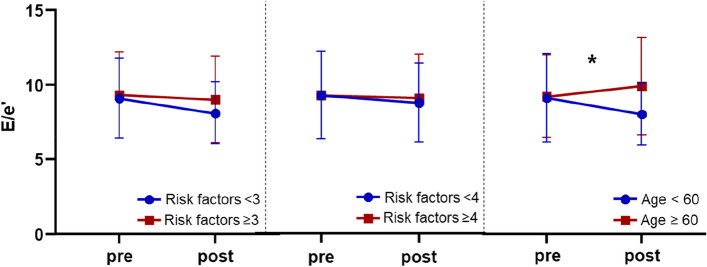
Results: Most patients (86.7%) had three or more cardiovascular risk factors, and about 32% had all five risk factors. Although the decrease in E/e' after the administration of SGLT2i was observed in 20% of enrolled patients, there was no significant difference in average E/e' value or left atrial volume index before and after the SGLT2i medication. Even in patients with all known risk factors including old age, E/e' value did not decrease after adding SGLT2i (8.9 ± 2.4 vs. 8.7 ± 3.2). There was a statistically significant difference in E/e' change after the SGLT2i administration between patients younger than 60 years and those older than 60 years (-0.7 ± 2.2 vs. 1.1 ± 2.8, P = 0.002).
Conclusions: In type 2 diabetes patients without documented cardiovascular disease including heart failure, administration of SGLT2i showed no improvement in diastolic function profile. Further large-scale randomized studies are needed to determine who will benefit from potential cardiovascular events with early addition of SGLT2i.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


