{"title":"Living Donor Liver Transplantation with Small Left Lobe Grafts: Prospective Validation of Utility of Splenectomy in Selected Recipients.","authors":"Hajime Matsushima, Akihiko Soyama, Takanobu Hara, Takashi Hamada, Yuta Kawaguchi, Kazushige Migita, Ayaka Satoh, Yamashita Mampei, Hajime Imamura, Ayaka Kinoshita, Tomohiko Adachi, Susumu Eguchi","doi":"10.12659/AOT.946374","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND We previously reported that the Model for End-stage Liver Disease (MELD) score and donor age are risk factors for small-for-size syndrome in adult living donor liver transplantation (LDLT) involving small grafts. Since April 2021, we have performed splenectomy as a portal inflow modulation in LDLT using small grafts according to the presence of risk factors. In this study, we evaluated the validity of our splenectomy strategies for optimizing graft outcomes. MATERIAL AND METHODS We retrospectively reviewed patients who underwent primary LDLT using left lobe grafts with the middle hepatic vein from January 2005 to January 2024 at our institution. We also compared the graft outcomes between recipients who underwent LDLT beginning in April 2021 (current policy group) and those who underwent LDLT in the era when splenectomy as portal modulation was not indicated (previous policy group). RESULTS In total, 173 consecutive LDLTs (current policy group: n=15) involving left lobe grafts were analyzed. Splenectomy was performed in 9 of 15 (60.0%) patients in the current policy group. All 15 patients in the current policy group remained alive for a median follow-up of 20.5 months. The rate of early allograft dysfunction was significantly lower, and the rate of small-for-size syndrome tended to be lower in the current policy group than in the previous policy group (13.3% vs 39.2%, P=0.047 and 20.0% vs 36.1%, P=0.211, respectively). CONCLUSIONS LDLT with splenectomy for high-risk patients may expand the availability of small left lobe grafts and optimize graft outcomes.</p>","PeriodicalId":7935,"journal":{"name":"Annals of Transplantation","volume":"30 ","pages":"e946374"},"PeriodicalIF":1.4000,"publicationDate":"2025-01-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11742235/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.12659/AOT.946374","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
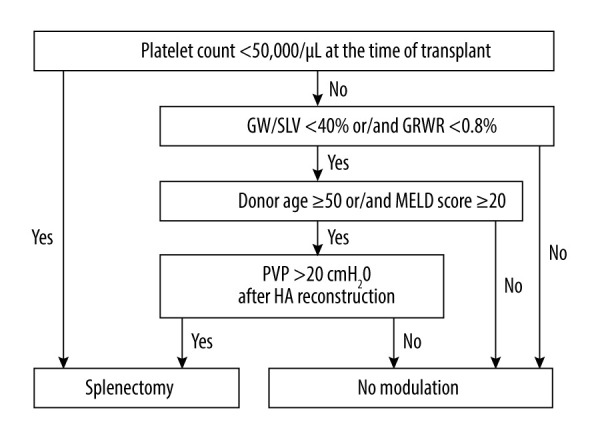
BACKGROUND We previously reported that the Model for End-stage Liver Disease (MELD) score and donor age are risk factors for small-for-size syndrome in adult living donor liver transplantation (LDLT) involving small grafts. Since April 2021, we have performed splenectomy as a portal inflow modulation in LDLT using small grafts according to the presence of risk factors. In this study, we evaluated the validity of our splenectomy strategies for optimizing graft outcomes. MATERIAL AND METHODS We retrospectively reviewed patients who underwent primary LDLT using left lobe grafts with the middle hepatic vein from January 2005 to January 2024 at our institution. We also compared the graft outcomes between recipients who underwent LDLT beginning in April 2021 (current policy group) and those who underwent LDLT in the era when splenectomy as portal modulation was not indicated (previous policy group). RESULTS In total, 173 consecutive LDLTs (current policy group: n=15) involving left lobe grafts were analyzed. Splenectomy was performed in 9 of 15 (60.0%) patients in the current policy group. All 15 patients in the current policy group remained alive for a median follow-up of 20.5 months. The rate of early allograft dysfunction was significantly lower, and the rate of small-for-size syndrome tended to be lower in the current policy group than in the previous policy group (13.3% vs 39.2%, P=0.047 and 20.0% vs 36.1%, P=0.211, respectively). CONCLUSIONS LDLT with splenectomy for high-risk patients may expand the availability of small left lobe grafts and optimize graft outcomes.
我们之前报道过终末期肝病模型(MELD)评分和供者年龄是涉及小移植物的成人活体供肝移植(LDLT)中小尺寸综合征的危险因素。自2021年4月以来,我们根据危险因素的存在,使用小移植物进行脾切除术作为LDLT的门静脉流入调节。在这项研究中,我们评估了脾切除术策略优化移植结果的有效性。材料和方法我们回顾性分析了2005年1月至2024年1月在我院接受肝中静脉左叶移植的原发性LDLT患者。我们还比较了从2021年4月开始接受LDLT的受体(现行政策组)和在没有脾切除术作为门静脉调节的时代接受LDLT的受体(以前的政策组)之间的移植结果。结果共分析了173例连续ldlt(当前政策组:n=15)涉及左叶移植物。现行政策组15例患者中有9例(60.0%)行脾切除术。现行政策组的所有15例患者中位随访时间为20.5个月。同种异体移植术后早期功能障碍发生率明显降低,小块综合征发生率有降低趋势(13.3% vs 39.2%, P=0.047; 20.0% vs 36.1%, P=0.211)。结论高危患者LDLT联合脾切除术可扩大小左叶移植的可用性并优化移植效果。
期刊介绍:
Annals of Transplantation is one of the fast-developing journals open to all scientists and fields of transplant medicine and related research. The journal is published quarterly and provides extensive coverage of the most important advances in transplantation.
Using an electronic on-line submission and peer review tracking system, Annals of Transplantation is committed to rapid review and publication. The average time to first decision is around 3-4 weeks. Time to publication of accepted manuscripts continues to be shortened, with the Editorial team committed to a goal of 3 months from acceptance to publication.
Expert reseachers and clinicians from around the world contribute original Articles, Review Papers, Case Reports and Special Reports in every pertinent specialty, providing a lot of arguments for discussion of exciting developments and controversies in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


