Rajendra Prasad Anne, Emine A Rahiman, Abhishek Somashekara Aradhya
{"title":"Real-time ultrasound for umbilical venous catheter insertion in neonates- a systematic review and meta-analysis.","authors":"Rajendra Prasad Anne, Emine A Rahiman, Abhishek Somashekara Aradhya","doi":"10.1186/s13089-025-00406-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>There has been an increase in real-time ultrasonography use in central venous catheterisation. This systematic review and meta-analysis aimed to assess the role of real-time ultrasound use in umbilical venous catheterisation in neonates.</p><p><strong>Data sources: </strong>PubMed, Embase, Web of Science and Cochrane Library were searched on July 11, 2024. We followed the Cochrane Handbook for Systematic Reviews of Interventions (for study conduct), GRADE methodology (for certainty of evidence), and PRISMA guidelines (for reporting).</p><p><strong>Study selection: </strong>All randomised controlled trials/RCTs and non-randomised studies of interventions/NRSIs comparing real-time ultrasound with the conventional technique of umbilical venous catheterisation were included.</p><p><strong>Data extraction: </strong>The outcomes of interest were malposition rates, procedure duration, mortality, sepsis, and cost. Data extraction and quality assessment were done in duplicate.</p><p><strong>Data synthesis: </strong>Six studies (three RCTs and three NRSI), including 863 participants, were included. Data were analysed separately for RCTs and NRSIs. The RCTs were at low risk of bias, but NRSIs were at moderate to serious risk. The pooled estimates from RCTs showed a decrease in malposition rates (2 studies, 165 participants, risk ratio/RR 0.45, 95% confidence interval/CI 0.23, 0.90) and procedure duration (3 studies, 196 participants, mean difference -6.1 min, 95% CI -8.4, -3.8 min) with real-time ultrasound use. There was no reduction in sepsis. Mortality was not reported. The certainty of evidence was low for malposition rates and procedure duration. The data from NRSIs showed a reduction in malposition rates (3 studies, 667 participants, risk ratio/RR 0.10, 95% confidence interval/CI 0.07, 0.14) without an impact on procedure duration and sepsis. However, these findings did not improve the evidence.</p><p><strong>Conclusions: </strong>Low certainty evidence suggests that using real-time ultrasound for umbilical venous catheterisation reduces malposition rates. There is a clinically insignificant reduction in procedure duration. There is no sufficient data to come to a conclusion on the critical outcomes of sepsis and mortality. PROSPERO registration number: CRD42024567895.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"17 1","pages":"4"},"PeriodicalIF":2.9000,"publicationDate":"2025-01-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11730037/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-025-00406-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: There has been an increase in real-time ultrasonography use in central venous catheterisation. This systematic review and meta-analysis aimed to assess the role of real-time ultrasound use in umbilical venous catheterisation in neonates.
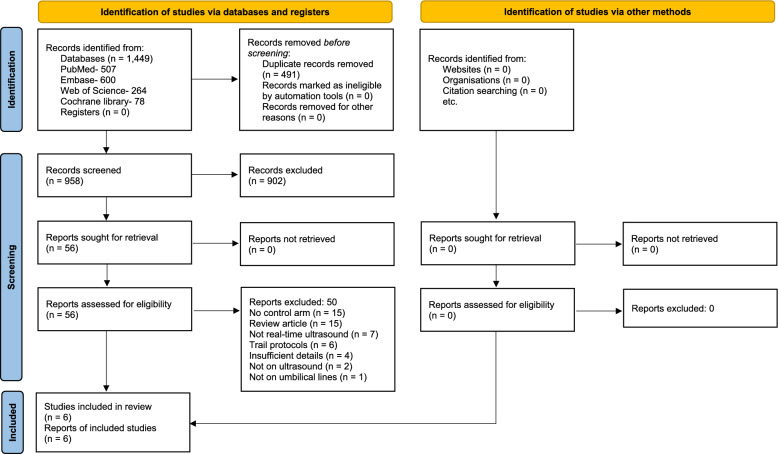
Data sources: PubMed, Embase, Web of Science and Cochrane Library were searched on July 11, 2024. We followed the Cochrane Handbook for Systematic Reviews of Interventions (for study conduct), GRADE methodology (for certainty of evidence), and PRISMA guidelines (for reporting).
Study selection: All randomised controlled trials/RCTs and non-randomised studies of interventions/NRSIs comparing real-time ultrasound with the conventional technique of umbilical venous catheterisation were included.
Data extraction: The outcomes of interest were malposition rates, procedure duration, mortality, sepsis, and cost. Data extraction and quality assessment were done in duplicate.
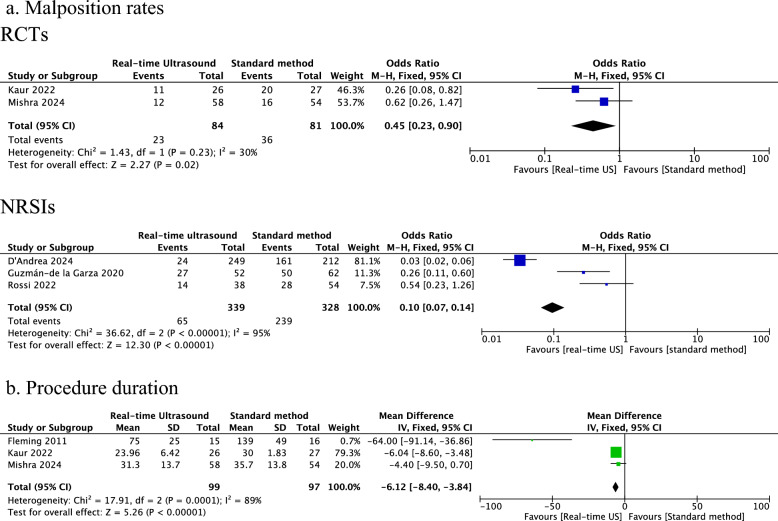
Data synthesis: Six studies (three RCTs and three NRSI), including 863 participants, were included. Data were analysed separately for RCTs and NRSIs. The RCTs were at low risk of bias, but NRSIs were at moderate to serious risk. The pooled estimates from RCTs showed a decrease in malposition rates (2 studies, 165 participants, risk ratio/RR 0.45, 95% confidence interval/CI 0.23, 0.90) and procedure duration (3 studies, 196 participants, mean difference -6.1 min, 95% CI -8.4, -3.8 min) with real-time ultrasound use. There was no reduction in sepsis. Mortality was not reported. The certainty of evidence was low for malposition rates and procedure duration. The data from NRSIs showed a reduction in malposition rates (3 studies, 667 participants, risk ratio/RR 0.10, 95% confidence interval/CI 0.07, 0.14) without an impact on procedure duration and sepsis. However, these findings did not improve the evidence.
Conclusions: Low certainty evidence suggests that using real-time ultrasound for umbilical venous catheterisation reduces malposition rates. There is a clinically insignificant reduction in procedure duration. There is no sufficient data to come to a conclusion on the critical outcomes of sepsis and mortality. PROSPERO registration number: CRD42024567895.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


