Nuria Olvera, Alvar Agusti, Judith M Vonk, Gang Wang, Jenny Hallberg, H Marike Boezen, Maarten van den Berge, Erik Melén, Rosa Faner
{"title":"Heterogeneity of reduced FEV<sub>1</sub> in early adulthood: A looking forward, looking backwards analysis.","authors":"Nuria Olvera, Alvar Agusti, Judith M Vonk, Gang Wang, Jenny Hallberg, H Marike Boezen, Maarten van den Berge, Erik Melén, Rosa Faner","doi":"10.1111/resp.14876","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Some individuals never achieve normal peak FEV<sub>1</sub> in early adulthood. It is unknown if this is due to airflow limitation and/or lung restriction.</p><p><strong>Methods: </strong>To investigate this, we: (1) looked forward in 19,791 participants in the Dutch Lifelines general population cohort aged 25-35 years with 5-year follow-up; and (2) looked backwards in 2032 participants in the Swedish BAMSE birth cohort with spirometry at 24 years of age but also at 16 and/or 8 years.</p><p><strong>Results: </strong>(1) In Lifelines 8.5% of participants had reduced FEV<sub>1</sub> at 25-35 years, 68% due to Preserved Ratio Impaired Spirometry ('PRISm') and 32% to airflow limitation ('low-limited'); besides, 3.8% participants with normal FEV<sub>1</sub> showed airflow-limitation ('normal-limited'). Low-limited and normal-limited, but not PRISm, reported higher smoking exposures and asthma diagnosis than normal (p < 0.05). At 5-year follow-up, 91.2% of participants remained in the same group, and FEV<sub>1</sub> decline was similar in normal and normal-limited participants, but statistically smaller (p < 0.05) in PRISm and low-limited; (2) these observations were largely reproduced in BAMSE at 24 years of age; and, (3) in BAMSE, low-limited or PRISm individuals were already identifiable at 8-16 years of age.</p><p><strong>Conclusion: </strong>Low peak FEV<sub>1</sub> in early adulthood is most often due to PRISm and results in a significant burden of respiratory symptoms. Only low-limited and normal-limited, but not PRISm, associate with a doctor diagnosis of asthma, and FEV<sub>1</sub> decline was statistically different in PRISm indicating a need for differentiated clinical approaches. These spirometric abnormalities can be already identified in childhood and adolescence.</p>","PeriodicalId":21129,"journal":{"name":"Respirology","volume":" ","pages":"326-334"},"PeriodicalIF":6.3000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11964992/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Respirology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/resp.14876","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/12 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Some individuals never achieve normal peak FEV1 in early adulthood. It is unknown if this is due to airflow limitation and/or lung restriction.
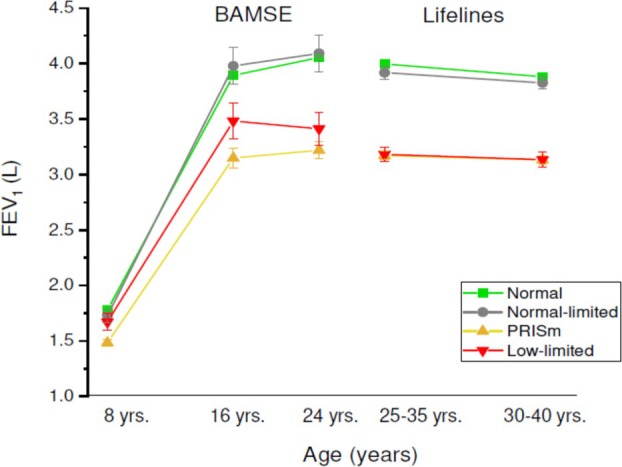
Methods: To investigate this, we: (1) looked forward in 19,791 participants in the Dutch Lifelines general population cohort aged 25-35 years with 5-year follow-up; and (2) looked backwards in 2032 participants in the Swedish BAMSE birth cohort with spirometry at 24 years of age but also at 16 and/or 8 years.
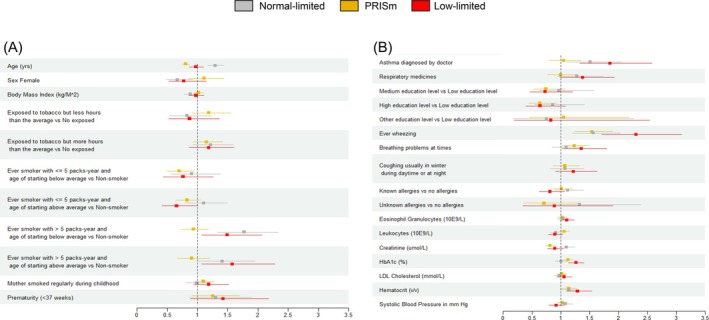
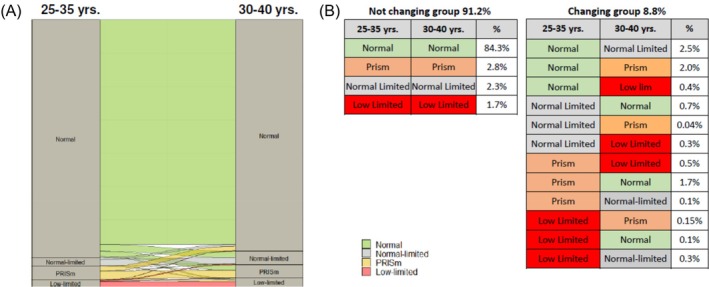
Results: (1) In Lifelines 8.5% of participants had reduced FEV1 at 25-35 years, 68% due to Preserved Ratio Impaired Spirometry ('PRISm') and 32% to airflow limitation ('low-limited'); besides, 3.8% participants with normal FEV1 showed airflow-limitation ('normal-limited'). Low-limited and normal-limited, but not PRISm, reported higher smoking exposures and asthma diagnosis than normal (p < 0.05). At 5-year follow-up, 91.2% of participants remained in the same group, and FEV1 decline was similar in normal and normal-limited participants, but statistically smaller (p < 0.05) in PRISm and low-limited; (2) these observations were largely reproduced in BAMSE at 24 years of age; and, (3) in BAMSE, low-limited or PRISm individuals were already identifiable at 8-16 years of age.
Conclusion: Low peak FEV1 in early adulthood is most often due to PRISm and results in a significant burden of respiratory symptoms. Only low-limited and normal-limited, but not PRISm, associate with a doctor diagnosis of asthma, and FEV1 decline was statistically different in PRISm indicating a need for differentiated clinical approaches. These spirometric abnormalities can be already identified in childhood and adolescence.
期刊介绍:
Respirology is a journal of international standing, publishing peer-reviewed articles of scientific excellence in clinical and clinically-relevant experimental respiratory biology and disease. Fields of research include immunology, intensive and critical care, epidemiology, cell and molecular biology, pathology, pharmacology, physiology, paediatric respiratory medicine, clinical trials, interventional pulmonology and thoracic surgery.
The Journal aims to encourage the international exchange of results and publishes papers in the following categories: Original Articles, Editorials, Reviews, and Correspondences.
Respirology is the preferred journal of the Thoracic Society of Australia and New Zealand, has been adopted as the preferred English journal of the Japanese Respiratory Society and the Taiwan Society of Pulmonary and Critical Care Medicine and is an official journal of the World Association for Bronchology and Interventional Pulmonology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


