{"title":"Best practices in the management of thyroid dysfunction induced by immune checkpoint inhibitors.","authors":"Ichiro Yamauchi, Daisuke Yabe","doi":"10.1530/ETJ-24-0328","DOIUrl":null,"url":null,"abstract":"<p><p>Immune checkpoint inhibitors (ICIs) frequently cause immune-related adverse events (irAEs), with thyroid irAEs being the most common endocrine-related irAEs. The incidence of overt thyroid irAEs was in the range of 8.9-22.2% in real-world settings, typically triggered by antibodies against PD-1 and PD-L1 and rarely by anti-CTLA-4 antibodies alone. The representative clinical course involves biphasic changes in thyroid function: transient thyrotoxicosis and subsequent persistent hypothyroidism. The identified risk factors for thyroid irAEs include the presence of thyroid autoantibodies, thyroid uptake on 18F-FDG-PET, prior use of tyrosine kinase inhibitors (TKIs), high BMI and high thyroid-stimulating hormone levels. There is evidence that overt thyroid irAEs are associated with good prognosis, at least in non-small cell lung cancer. Although the clinical features have been well clarified, the management strategies require further refinement. Routine monitoring of thyroid function every 4-6 weeks during ICI therapy is recommended for early detection of thyroid irAEs. While thyrotoxicosis generally requires observation only, hypothyroidism should be promptly treated with levothyroxine replacement. Continuation of ICI therapy is typically feasible in patients with thyroid irAEs, provided their overall health remains stable. However, these strategies were largely based on clinical experience with monotherapy. As combination ICI therapies have been developed as first-line treatments, antitumor agents may modify the clinical features of thyroid irAEs. For example, cytotoxic agents can delay the onset of thyroid irAEs, while TKIs are often linked to early-onset hypothyroidism, independent of ICI use. Given the increasing diversity and complexity of cancer immunotherapy, it is essential to vigilantly screen for thyroid irAEs.</p>","PeriodicalId":12159,"journal":{"name":"European Thyroid Journal","volume":" ","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2025-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11816041/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Thyroid Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1530/ETJ-24-0328","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
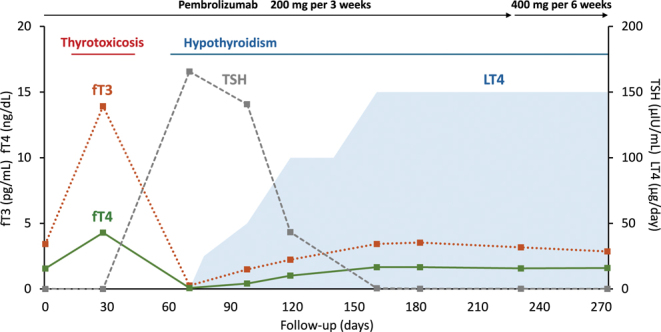
Immune checkpoint inhibitors (ICIs) frequently cause immune-related adverse events (irAEs), with thyroid irAEs being the most common endocrine-related irAEs. The incidence of overt thyroid irAEs was in the range of 8.9-22.2% in real-world settings, typically triggered by antibodies against PD-1 and PD-L1 and rarely by anti-CTLA-4 antibodies alone. The representative clinical course involves biphasic changes in thyroid function: transient thyrotoxicosis and subsequent persistent hypothyroidism. The identified risk factors for thyroid irAEs include the presence of thyroid autoantibodies, thyroid uptake on 18F-FDG-PET, prior use of tyrosine kinase inhibitors (TKIs), high BMI and high thyroid-stimulating hormone levels. There is evidence that overt thyroid irAEs are associated with good prognosis, at least in non-small cell lung cancer. Although the clinical features have been well clarified, the management strategies require further refinement. Routine monitoring of thyroid function every 4-6 weeks during ICI therapy is recommended for early detection of thyroid irAEs. While thyrotoxicosis generally requires observation only, hypothyroidism should be promptly treated with levothyroxine replacement. Continuation of ICI therapy is typically feasible in patients with thyroid irAEs, provided their overall health remains stable. However, these strategies were largely based on clinical experience with monotherapy. As combination ICI therapies have been developed as first-line treatments, antitumor agents may modify the clinical features of thyroid irAEs. For example, cytotoxic agents can delay the onset of thyroid irAEs, while TKIs are often linked to early-onset hypothyroidism, independent of ICI use. Given the increasing diversity and complexity of cancer immunotherapy, it is essential to vigilantly screen for thyroid irAEs.
期刊介绍:
The ''European Thyroid Journal'' publishes papers reporting original research in basic, translational and clinical thyroidology. Original contributions cover all aspects of the field, from molecular and cellular biology to immunology and biochemistry, from physiology to pathology, and from pediatric to adult thyroid diseases with a special focus on thyroid cancer. Readers also benefit from reviews by noted experts, which highlight especially active areas of current research. The journal will further publish formal guidelines in the field, produced and endorsed by the European Thyroid Association.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


