Amit Saxena, Cristina Sorrento, Peter Izmirly, Janine Sullivan, Monica Gamez-Perez, Jammie Law, Howard Michael Belmont, Jill P Buyon
{"title":"Low versus high initial oral glucocorticoid dose for lupus nephritis: a pooled analysis of randomised controlled clinical trials.","authors":"Amit Saxena, Cristina Sorrento, Peter Izmirly, Janine Sullivan, Monica Gamez-Perez, Jammie Law, Howard Michael Belmont, Jill P Buyon","doi":"10.1136/lupus-2024-001351","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Traditional initial treatment regimens for lupus nephritis (LN) used oral glucocorticoids (GC) in starting doses up to 1.0 mg/kg/day prednisone equivalent with or without a preceding intravenous methylprednisolone pulse. More recent management guidelines recommend lower starting oral GC doses following intravenous pulse therapy. As there have been no large studies directly comparing patients receiving low versus high initial oral GC doses, this pooled analysis of high-quality randomised controlled trials (RCTs) aims to evaluate differences in efficacy and safety.</p><p><strong>Methods: </strong>Published data were analysed from RCTs that assessed variable GC doses in the standard of care (SOC) treatment arms. Patients receiving starting prednisone doses up to 0.5 mg/kg/day (low dose) were compared with 1.0 mg/kg/day (high dose). Complete renal response requiring urine protein-creatinine ratio <0.5 mg/mg (CRR 0.5), CRR or partial renal response (PRR), serious adverse events (SAE) and SAE due to infections at 12 months of treatment were compared between groups.</p><p><strong>Results: </strong>417 patients from SOC arms of five studies were exposed to low-dose initial GC after intravenous pulse, while 521 patients from four studies were treated with high-dose oral GC. In patients with low-dose oral GC, 25.2% achieved CRR 0.5 at 12 months compared with 27.2% in high-dose groups, p=0.54. CRR or PRR was attained in 48.7% low-dose vs 43.6% high-dose patients, p=0.14. SAEs and infection SAEs were less common in the low-dose GC group (19.4% vs 31.6%, p<0.001 and 9.8% vs 16.5%, p=0.012, respectively).</p><p><strong>Conclusions: </strong>Based on pooled RCT data, there was no significant difference in 12-month renal responses between patients receiving low-dose prednisone following intravenous GC compared with those receiving initial high doses. SAEs were less frequent in patients receiving low-dose initial GC. These findings support the use of lower oral GC doses in LN treatment.</p>","PeriodicalId":18126,"journal":{"name":"Lupus Science & Medicine","volume":"12 1","pages":""},"PeriodicalIF":3.5000,"publicationDate":"2025-01-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11752037/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lupus Science & Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/lupus-2024-001351","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Traditional initial treatment regimens for lupus nephritis (LN) used oral glucocorticoids (GC) in starting doses up to 1.0 mg/kg/day prednisone equivalent with or without a preceding intravenous methylprednisolone pulse. More recent management guidelines recommend lower starting oral GC doses following intravenous pulse therapy. As there have been no large studies directly comparing patients receiving low versus high initial oral GC doses, this pooled analysis of high-quality randomised controlled trials (RCTs) aims to evaluate differences in efficacy and safety.
Methods: Published data were analysed from RCTs that assessed variable GC doses in the standard of care (SOC) treatment arms. Patients receiving starting prednisone doses up to 0.5 mg/kg/day (low dose) were compared with 1.0 mg/kg/day (high dose). Complete renal response requiring urine protein-creatinine ratio <0.5 mg/mg (CRR 0.5), CRR or partial renal response (PRR), serious adverse events (SAE) and SAE due to infections at 12 months of treatment were compared between groups.
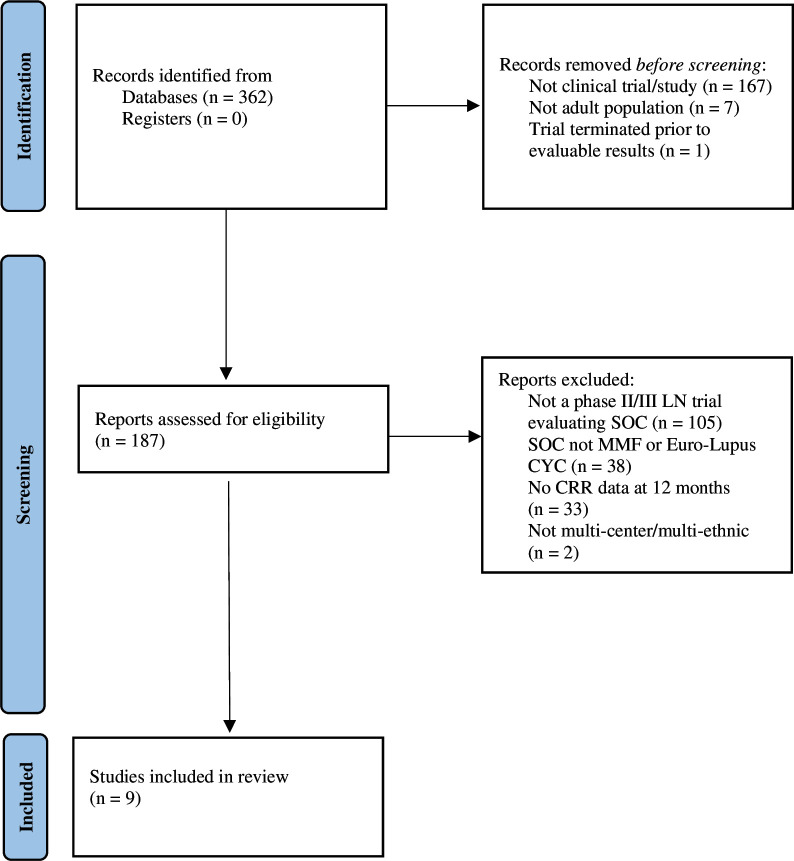
Results: 417 patients from SOC arms of five studies were exposed to low-dose initial GC after intravenous pulse, while 521 patients from four studies were treated with high-dose oral GC. In patients with low-dose oral GC, 25.2% achieved CRR 0.5 at 12 months compared with 27.2% in high-dose groups, p=0.54. CRR or PRR was attained in 48.7% low-dose vs 43.6% high-dose patients, p=0.14. SAEs and infection SAEs were less common in the low-dose GC group (19.4% vs 31.6%, p<0.001 and 9.8% vs 16.5%, p=0.012, respectively).
Conclusions: Based on pooled RCT data, there was no significant difference in 12-month renal responses between patients receiving low-dose prednisone following intravenous GC compared with those receiving initial high doses. SAEs were less frequent in patients receiving low-dose initial GC. These findings support the use of lower oral GC doses in LN treatment.
期刊介绍:
Lupus Science & Medicine is a global, peer reviewed, open access online journal that provides a central point for publication of basic, clinical, translational, and epidemiological studies of all aspects of lupus and related diseases. It is the first lupus-specific open access journal in the world and was developed in response to the need for a barrier-free forum for publication of groundbreaking studies in lupus. The journal publishes research on lupus from fields including, but not limited to: rheumatology, dermatology, nephrology, immunology, pediatrics, cardiology, hepatology, pulmonology, obstetrics and gynecology, and psychiatry.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


