Tumour necrosis factor inhibitors in Ulcerative colitis: real-world data on Therapeutic drug monitoring and evaluation of current treatment targets (STRIDE II).
Jonas Andre Lundekvam, Marte Lie Høivik, Karoline Anisdahl, Milada Cvancarova Småstuen, David J Warren, Nils Bolstad, Asle Wilhelm Medhus
{"title":"Tumour necrosis factor inhibitors in Ulcerative colitis: real-world data on Therapeutic drug monitoring and evaluation of current treatment targets (STRIDE II).","authors":"Jonas Andre Lundekvam, Marte Lie Høivik, Karoline Anisdahl, Milada Cvancarova Småstuen, David J Warren, Nils Bolstad, Asle Wilhelm Medhus","doi":"10.1080/07853890.2024.2424447","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The benefit of therapeutic drug monitoring (TDM) and implementation of recommendations from the Selection of Therapeutic Targets in Inflammatory Bowel Disease (IBD, STRIDE) are discussed in the IBD community. We report real-world data in ulcerative colitis patients receiving first-line tumour necrosis factor inhibitor (TNFi) treatment followed by TDM, and assess how implementation of the STRIDE II recommendations might affect clinical practice.</p><p><strong>Methods: </strong>Adult, biologically naïve UC patients starting TNFi between 2014 and 2021 at Oslo University Hospital were included in a medical chart review study, and data were collected at three and twelve months after the start of treatment. Target serum drug levels were defined as ≥7.5 mg/L for adalimumab and ≥5 mg/L for infliximab.</p><p><strong>Results: </strong>Of 141 included patients, 36% were in clinical and biochemical (combined) remission after twelve months. Among 102 treatment persistent patients, 54% were in combined remission after twelve months. Target drug level at three months was associated with clinical remission at twelve months (OR = 2.97, 95% CI [1.24-7.12]) and biochemical remission at twelve months (OR = 2.64, 95% CI [1.03-6.77]). In total, 56% of recorded dosage adjustments were related only to serum drug levels.</p><p><strong>Conclusions: </strong>Combined remission rates at twelve months for treatment persistent patients suggest that 46% should have been considered for a change of treatment according to the STRIDE II recommendations. A majority of dosage adjustments were made proactively. Target drug level at three months was associated with remission at twelve months and supports the use of proactive TDM.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2424447"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11721610/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2024.2424447","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/6 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The benefit of therapeutic drug monitoring (TDM) and implementation of recommendations from the Selection of Therapeutic Targets in Inflammatory Bowel Disease (IBD, STRIDE) are discussed in the IBD community. We report real-world data in ulcerative colitis patients receiving first-line tumour necrosis factor inhibitor (TNFi) treatment followed by TDM, and assess how implementation of the STRIDE II recommendations might affect clinical practice.
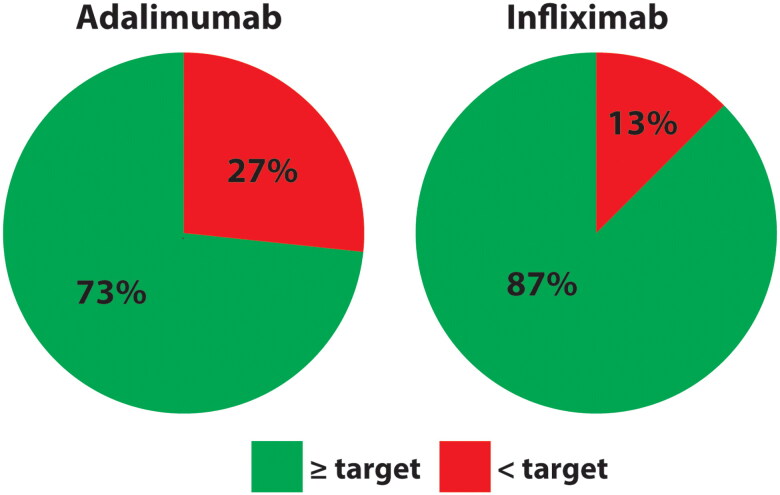
Methods: Adult, biologically naïve UC patients starting TNFi between 2014 and 2021 at Oslo University Hospital were included in a medical chart review study, and data were collected at three and twelve months after the start of treatment. Target serum drug levels were defined as ≥7.5 mg/L for adalimumab and ≥5 mg/L for infliximab.
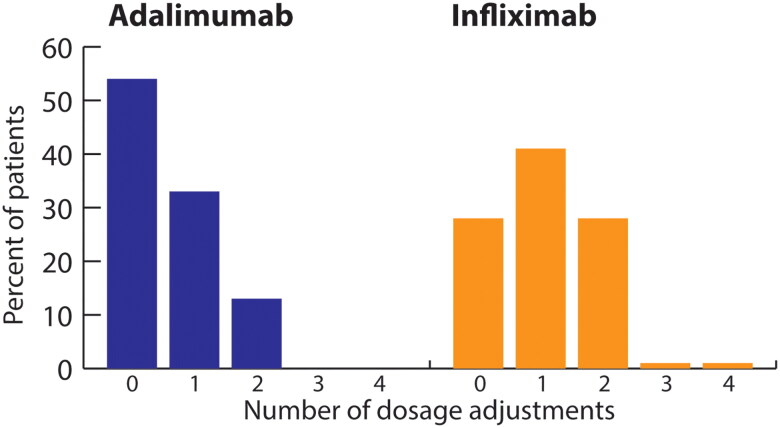
Results: Of 141 included patients, 36% were in clinical and biochemical (combined) remission after twelve months. Among 102 treatment persistent patients, 54% were in combined remission after twelve months. Target drug level at three months was associated with clinical remission at twelve months (OR = 2.97, 95% CI [1.24-7.12]) and biochemical remission at twelve months (OR = 2.64, 95% CI [1.03-6.77]). In total, 56% of recorded dosage adjustments were related only to serum drug levels.
Conclusions: Combined remission rates at twelve months for treatment persistent patients suggest that 46% should have been considered for a change of treatment according to the STRIDE II recommendations. A majority of dosage adjustments were made proactively. Target drug level at three months was associated with remission at twelve months and supports the use of proactive TDM.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


