A rare case of Gardnerella vaginalis spondylodiscitis
IF 1
Q4 INFECTIOUS DISEASES
引用次数: 0
Abstract
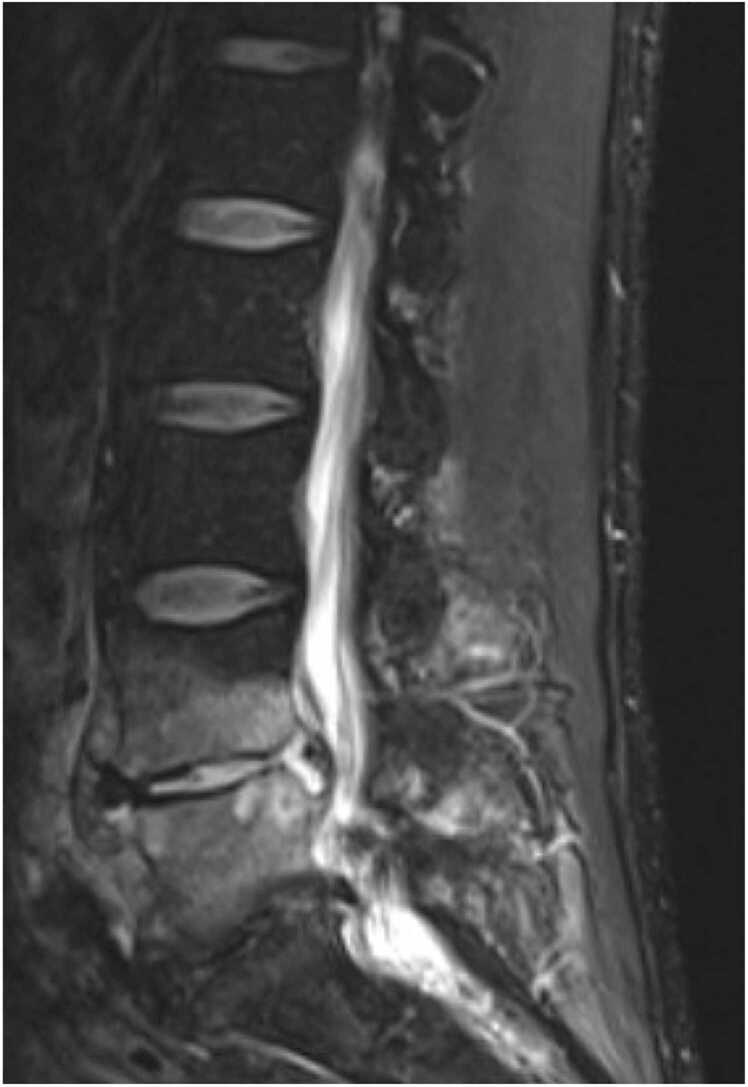
A 55-year-old-male with a chronic left uretero-pelvic junction (UPJ) obstruction managed with intermittent stent exchanges presented with low midline back pain. CT Abdomen/Pelvis revealed spondylodiscitis at L4-L5, further demonstrated on MRI Lumbar spine. Imaging also revealed the left nephro-ureteral stent was mispositioned, with some mild wall thickening of the left ureter. He was not systemically ill, and antimicrobials were held. He underwent a L4/5 disc biopsy, and pathology revealed acute discitis. Blood and biopsy cultures remained negative through hospital day 5. He then underwent repeat L4/5 disc biopsy. Cultures of repeat biopsy resulted in Gardnerella vaginalis. IV antimicrobials were stopped, and oral Metronidazole was started. He completed 10 weeks of Metronidazole therapy, with significant clinical improvement.
G. vaginalis is a rare cause of bone and joint infections. It is difficult to culture and is less virulent than common bacteria associated with native vertebral osteomyelitis. There have been few case reports of G. vaginalis osteomyelitis or prosthetic joint infection, especially in males. G. vaginalis can rarely colonize the urethra in men and has been known to form biofilm on foreign material in the female genitourinary system. We suspect our patient had developed colonization of his ureteral stent, predisposing him to osteomyelitis. Were repeat biopsy not pursued in this case, our patient likely could have developed empiric treatment failure. Holding antibiotics after initial biopsy proved highly beneficial.
罕见的阴道加德纳菌性脊柱炎1例。
55岁男性慢性左输尿管-骨盆连接处(UPJ)梗阻,间歇性支架置换后出现腰中线疼痛。腹部/骨盆CT显示L4-L5椎板椎间盘炎,腰椎MRI进一步证实。影像也显示左侧肾输尿管支架位置不正确,左侧输尿管壁轻度增厚。他没有全身性疾病,而且还服用了抗菌剂。他接受了L4/5椎间盘活检,病理显示急性椎间盘炎。入院第5天,血液和活检培养均为阴性。然后再次行L4/5椎间盘活检。重复活检培养结果为阴道加德纳菌。停止静脉注射抗微生物药物,开始口服甲硝唑。完成10周甲硝唑治疗,临床明显改善。阴道炎是一种罕见的骨和关节感染的原因。它很难培养,毒性低于与原生椎体骨髓炎相关的常见细菌。阴道支原体骨髓炎或假体关节感染的病例报道很少,尤其是在男性中。阴道芽孢杆菌很少在男性尿道中定植,在女性泌尿生殖系统的异物上形成生物膜。我们怀疑病人的输尿管支架已形成定植,使他易患骨髓炎。如果在本病例中没有进行重复活检,我们的患者可能会出现经验性治疗失败。初步活检后服用抗生素证明是非常有益的。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


