Jonathan N Le, Jordan O Gasho, Olivia Peony, Asneh Singh, Katrina D Silos, Sungjin Kim, Anthony T Nguyen, Mitchell Kamrava, Amin Mirhadi, Behrooz Hakimian, Karen L Reckamp, Kamya Sankar, Raymond H Mak, Andriana P Nikolova, Katelyn M Atkins
{"title":"Cardiac events and dynamic echocardiographic and electrocardiogram changes following osimertinib treatment in lung cancer.","authors":"Jonathan N Le, Jordan O Gasho, Olivia Peony, Asneh Singh, Katrina D Silos, Sungjin Kim, Anthony T Nguyen, Mitchell Kamrava, Amin Mirhadi, Behrooz Hakimian, Karen L Reckamp, Kamya Sankar, Raymond H Mak, Andriana P Nikolova, Katelyn M Atkins","doi":"10.3389/fcvm.2024.1485033","DOIUrl":null,"url":null,"abstract":"<p><p>Osimertinib is first-line treatment for epidermal growth factor (EGFR)-mutated non-small cell lung cancer (NSCLC) and has been associated with cardiotoxicity. However, the nature of cardiac remodeling and associated risk factors remains incompletely understood. Retrospective analysis of NSCLC patients with ≥1 echocardiogram post-osimertinib between 2007 and 2022 was performed. The cumulative incidence of grade ≥2 cardiac common terminology criteria for adverse events (CTCAE) was estimated and Fine and Gray regressions performed (non-cardiac death as competing risk). Eighty-five patients [mean [interquartile range, IQR], 68 [60-75] years; 67% female; 12% with pre-existing heart conditions] met inclusion criteria. With a median follow up of 34.7 months, the 2-year cumulative incidence of grade ≥2 and grade ≥3 cardiac events were 19.2% and 8.5%, respectively. There was an increased risk of grade ≥2 cardiac CTCAE with pre-existing arrhythmia [hazard ratio(HR) 3.90, 95%CI, 1.11-13.72; <i>p</i> = 0.034] and higher body mass index (HR 1.07, 95%CI, 1.00-1.14; <i>p</i> = 0.04). Following osimertinib (vs. baseline), the median QTc was prolonged (451 vs. 437 ms; <i>p</i> < 0.001) and LVEF ≤50% was more common (10.6% vs. 5.3%; <i>p</i> = .046). Osimertinib treatment was associated with QTc prolongation and reduced LVEF. BMI was identified as a potentially modifiable risk factor for osimertinib-associated cardiotoxicity, worthy of further study.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"11 ","pages":"1485033"},"PeriodicalIF":2.8000,"publicationDate":"2024-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11685755/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2024.1485033","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
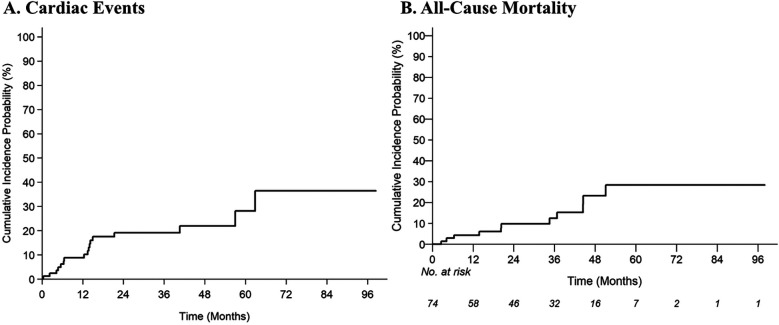
Osimertinib is first-line treatment for epidermal growth factor (EGFR)-mutated non-small cell lung cancer (NSCLC) and has been associated with cardiotoxicity. However, the nature of cardiac remodeling and associated risk factors remains incompletely understood. Retrospective analysis of NSCLC patients with ≥1 echocardiogram post-osimertinib between 2007 and 2022 was performed. The cumulative incidence of grade ≥2 cardiac common terminology criteria for adverse events (CTCAE) was estimated and Fine and Gray regressions performed (non-cardiac death as competing risk). Eighty-five patients [mean [interquartile range, IQR], 68 [60-75] years; 67% female; 12% with pre-existing heart conditions] met inclusion criteria. With a median follow up of 34.7 months, the 2-year cumulative incidence of grade ≥2 and grade ≥3 cardiac events were 19.2% and 8.5%, respectively. There was an increased risk of grade ≥2 cardiac CTCAE with pre-existing arrhythmia [hazard ratio(HR) 3.90, 95%CI, 1.11-13.72; p = 0.034] and higher body mass index (HR 1.07, 95%CI, 1.00-1.14; p = 0.04). Following osimertinib (vs. baseline), the median QTc was prolonged (451 vs. 437 ms; p < 0.001) and LVEF ≤50% was more common (10.6% vs. 5.3%; p = .046). Osimertinib treatment was associated with QTc prolongation and reduced LVEF. BMI was identified as a potentially modifiable risk factor for osimertinib-associated cardiotoxicity, worthy of further study.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


