Tarik Hadid, Adam Biedny, Hirva Mamdani, Asfar Azmi, Seongho Kim, Hyejeong Jang, Dipesh Uprety, Mohammed Najeeb Al Hallak, Ammar Sukari
{"title":"Association between cannabis use and clinical outcomes in patients with solid malignancies receiving immune checkpoint inhibitors.","authors":"Tarik Hadid, Adam Biedny, Hirva Mamdani, Asfar Azmi, Seongho Kim, Hyejeong Jang, Dipesh Uprety, Mohammed Najeeb Al Hallak, Ammar Sukari","doi":"10.1177/25151355241309095","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cannabis (CAN) use has risen significantly over the last few decades. CAN has potent immunosuppressive properties, which could antagonize the effect of immunotherapy (IO). The impact of CAN use on clinical cancer outcomes remains unclear.</p><p><strong>Objectives: </strong>In this study, we evaluated the clinical effect of CAN use on clinical outcomes among patients with solid malignancies receiving IO.</p><p><strong>Design: </strong>This is a retrospective cohort study of all patients with solid malignancies receiving IO between August 2014 and August 2018.</p><p><strong>Methods: </strong>Patients were stratified based on CAN use to CAN users and CAN non-users. The primary outcome was overall survival (OS), and the secondary outcomes were progression-free survival (PFS) and disease control rate (DCR). Univariable and multivariable logistic and Cox regression analyses were performed to compare the outcomes between the two groups, adjusting for covariates.</p><p><strong>Results: </strong>The records of 106 patients were reviewed, 28 (26%) of whom were CAN users and 78 (74%) were CAN non-users. One patient was excluded. Most CAN users consumed dronabinol (82%). The median follow-up for OS and PFS was 29.2 months. Median OS in the CAN users was 6.7 months compared to 17.3 months in the CAN non-users (HR, 1.78; 95% CI, 1.06-2.97; <i>p</i> = 0.029). The median PFS was 4.8 months in the CAN users compared to 9.7 months in the CAN non-users (HR, 1.74; 95% CI, 1.09-2.79; <i>p</i> = 0.021). DCR was 11% among CAN users and 38% among CAN non-users (OR, 0.23; 95% CI; 0.06-0.68; <i>p</i> = 0.007). An exploratory racial disparity analysis showed that this negative impact of CAN was primarily seen in White patients.</p><p><strong>Conclusion: </strong>In this single institutional experience, CAN use was associated with worse OS, PFS, and DCR among cancer patients receiving IO. Prospective trials are needed to further study this potential antagonistic interaction between CAN and IO and explore the racial disparities related to CAN exposure.</p>","PeriodicalId":33285,"journal":{"name":"Therapeutic Advances in Vaccines and Immunotherapy","volume":"12 ","pages":"25151355241309095"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683815/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Vaccines and Immunotherapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/25151355241309095","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cannabis (CAN) use has risen significantly over the last few decades. CAN has potent immunosuppressive properties, which could antagonize the effect of immunotherapy (IO). The impact of CAN use on clinical cancer outcomes remains unclear.
Objectives: In this study, we evaluated the clinical effect of CAN use on clinical outcomes among patients with solid malignancies receiving IO.
Design: This is a retrospective cohort study of all patients with solid malignancies receiving IO between August 2014 and August 2018.
Methods: Patients were stratified based on CAN use to CAN users and CAN non-users. The primary outcome was overall survival (OS), and the secondary outcomes were progression-free survival (PFS) and disease control rate (DCR). Univariable and multivariable logistic and Cox regression analyses were performed to compare the outcomes between the two groups, adjusting for covariates.
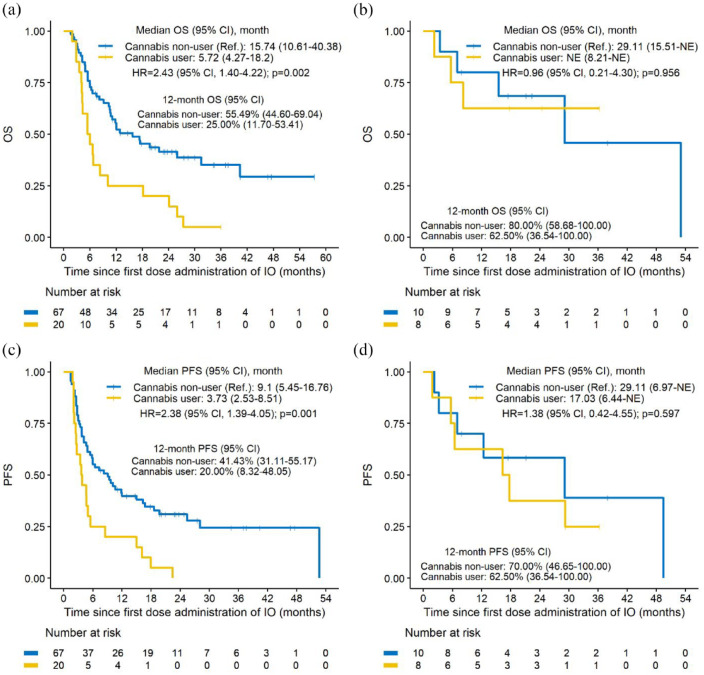
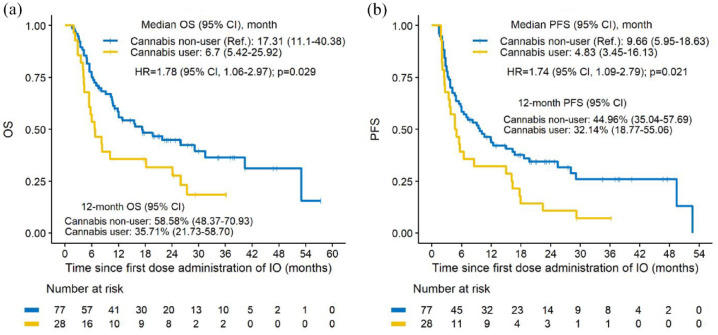
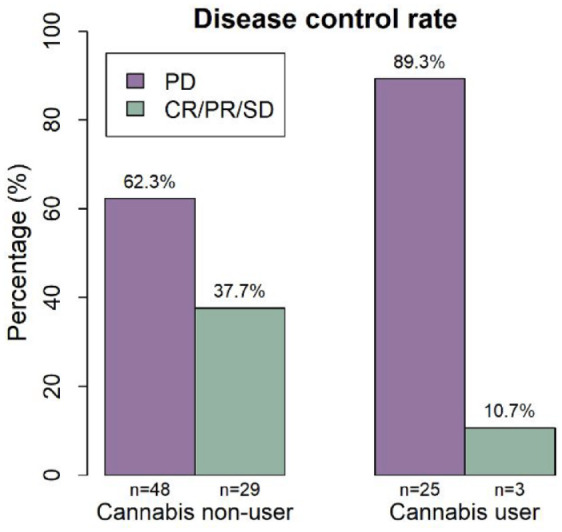
Results: The records of 106 patients were reviewed, 28 (26%) of whom were CAN users and 78 (74%) were CAN non-users. One patient was excluded. Most CAN users consumed dronabinol (82%). The median follow-up for OS and PFS was 29.2 months. Median OS in the CAN users was 6.7 months compared to 17.3 months in the CAN non-users (HR, 1.78; 95% CI, 1.06-2.97; p = 0.029). The median PFS was 4.8 months in the CAN users compared to 9.7 months in the CAN non-users (HR, 1.74; 95% CI, 1.09-2.79; p = 0.021). DCR was 11% among CAN users and 38% among CAN non-users (OR, 0.23; 95% CI; 0.06-0.68; p = 0.007). An exploratory racial disparity analysis showed that this negative impact of CAN was primarily seen in White patients.
Conclusion: In this single institutional experience, CAN use was associated with worse OS, PFS, and DCR among cancer patients receiving IO. Prospective trials are needed to further study this potential antagonistic interaction between CAN and IO and explore the racial disparities related to CAN exposure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


