Laura H Kim, Marisa Catapang, Nonnie Polderman, Robert Humphreys, Cherry Mammen, Eleonora Jugnauth, Douglas G Matsell
{"title":"Outcomes Using a Standardized Provincial Childhood Nephrotic Syndrome Clinical Pathway.","authors":"Laura H Kim, Marisa Catapang, Nonnie Polderman, Robert Humphreys, Cherry Mammen, Eleonora Jugnauth, Douglas G Matsell","doi":"10.1177/20543581241304505","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In 2013, the British Columbia (BC) Childhood Nephrotic Syndrome Clinical Pathway (CNSCP) was developed to standardize the care of children with nephrotic syndrome (NS). In BC, children access nephrology care at BC Children's Hospital (BCCH) and multiple regional clinics.</p><p><strong>Objective: </strong>The primary objective was to compare induction therapy and clinical outcomes between BCCH and regional clinics since implementation of the CNSCP.</p><p><strong>Design setting and patients: </strong>This was a retrospective cohort study of children with NS in BC.</p><p><strong>Measurements and methods: </strong>We conducted a retrospective cohort study of children 1 to 17 years old with new-onset NS from 2013 to 2019 inclusive with minimum 12 months of follow-up. Children with non-minimal change disease, steroid resistance, incomplete induction therapy, or less than 6 months of pathway treatment within their first year post-diagnosis were excluded. Clinics were categorized as BCCH or regional (Surrey, Prince George, or Kelowna).</p><p><strong>Results: </strong>Sixty-nine patients were included, with 52 (75%) at BCCH and 17 (25%) at regional clinics. There were no significant between-group differences in age, sex, or clinical characteristics at time of diagnosis. Comparing BCCH and regional clinics, there was no difference in induction prednisone exposure (median 3400, interquartile range [IQR] 3331-3585 mg/m<sup>2</sup> vs 3492, IQR 3397-3644 mg/m<sup>2</sup>, <i>P</i> = .167), annualized relapse rate (median 3.3, IQR 1.1-5.3 vs 2.3, IQR 0.5-4.2, <i>P</i> = .575), or development of frequently relapsing courses (50% vs 62%, <i>P</i> = .475). There was a similar number of first-year clinic visits (4.2 ± 1.2 vs 4.0 ± 1.8, <i>P</i> = .655) and dietitian-reviewed food records (67% vs 47%, <i>P</i> = .135, BCCH vs regional). More children at BCCH had a recommended ophthalmology surveillance visit (87% vs 59%, <i>P</i> = .01, BCCH vs regional).</p><p><strong>Limitations: </strong>Study limitations include small sample size and exclusion of children with complicated NS (ie, relapse during induction, steroid resistance).</p><p><strong>Conclusion: </strong>Since we implemented the CNSCP, children with NS received comparable care and had similar outcomes at BCCH and regional clinics without significant practice variation.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241304505"},"PeriodicalIF":1.5000,"publicationDate":"2024-12-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683811/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241304505","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
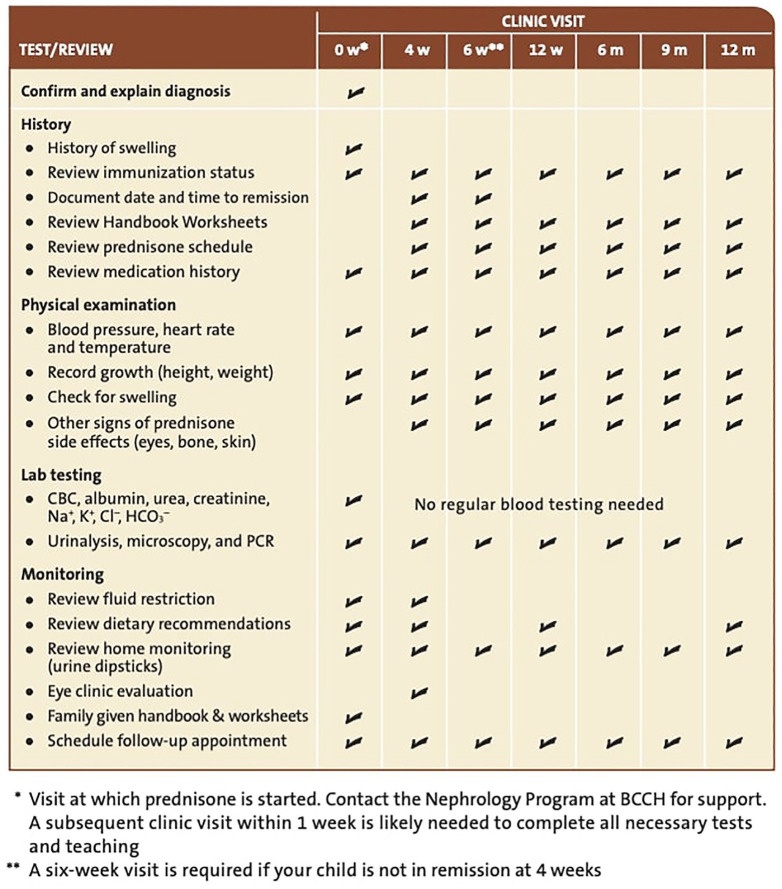
Background: In 2013, the British Columbia (BC) Childhood Nephrotic Syndrome Clinical Pathway (CNSCP) was developed to standardize the care of children with nephrotic syndrome (NS). In BC, children access nephrology care at BC Children's Hospital (BCCH) and multiple regional clinics.
Objective: The primary objective was to compare induction therapy and clinical outcomes between BCCH and regional clinics since implementation of the CNSCP.
Design setting and patients: This was a retrospective cohort study of children with NS in BC.
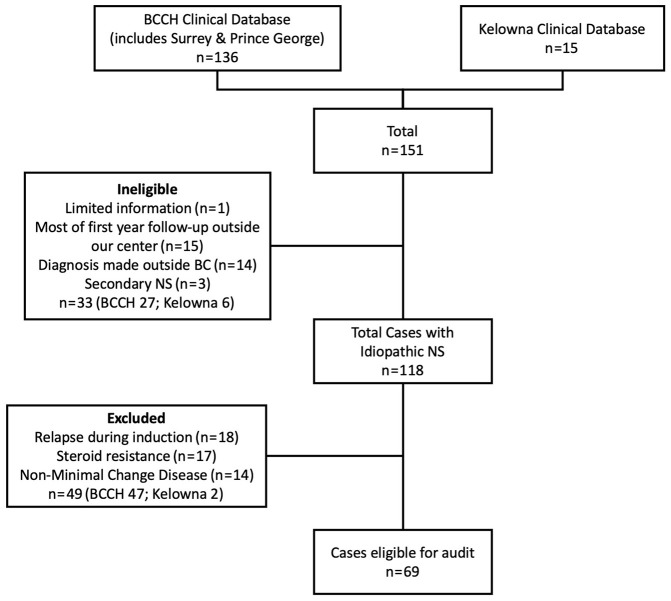
Measurements and methods: We conducted a retrospective cohort study of children 1 to 17 years old with new-onset NS from 2013 to 2019 inclusive with minimum 12 months of follow-up. Children with non-minimal change disease, steroid resistance, incomplete induction therapy, or less than 6 months of pathway treatment within their first year post-diagnosis were excluded. Clinics were categorized as BCCH or regional (Surrey, Prince George, or Kelowna).
Results: Sixty-nine patients were included, with 52 (75%) at BCCH and 17 (25%) at regional clinics. There were no significant between-group differences in age, sex, or clinical characteristics at time of diagnosis. Comparing BCCH and regional clinics, there was no difference in induction prednisone exposure (median 3400, interquartile range [IQR] 3331-3585 mg/m2 vs 3492, IQR 3397-3644 mg/m2, P = .167), annualized relapse rate (median 3.3, IQR 1.1-5.3 vs 2.3, IQR 0.5-4.2, P = .575), or development of frequently relapsing courses (50% vs 62%, P = .475). There was a similar number of first-year clinic visits (4.2 ± 1.2 vs 4.0 ± 1.8, P = .655) and dietitian-reviewed food records (67% vs 47%, P = .135, BCCH vs regional). More children at BCCH had a recommended ophthalmology surveillance visit (87% vs 59%, P = .01, BCCH vs regional).
Limitations: Study limitations include small sample size and exclusion of children with complicated NS (ie, relapse during induction, steroid resistance).
Conclusion: Since we implemented the CNSCP, children with NS received comparable care and had similar outcomes at BCCH and regional clinics without significant practice variation.
背景:2013年,不列颠哥伦比亚省(BC)制定了儿童肾病综合征临床路径(CNSCP),以规范儿童肾病综合征(NS)的护理。在不列颠哥伦比亚省,儿童可以在不列颠哥伦比亚省儿童医院(BCCH)和多个地区诊所接受肾脏病治疗。目的:主要目的是比较自CNSCP实施以来,BCCH和区域诊所的诱导治疗和临床结果。设计环境和患者:这是一项针对不列颠哥伦比亚省NS患儿的回顾性队列研究。测量和方法:我们对2013年至2019年1至17岁新发NS患儿进行了回顾性队列研究,随访时间至少为12个月。排除非最小变化疾病、类固醇抵抗、不完全诱导治疗或诊断后一年内途径治疗少于6个月的儿童。诊所被分类为BCCH或区域(萨里、乔治王子或基洛纳)。结果:纳入69例患者,其中52例(75%)在BCCH就诊,17例(25%)在区域诊所就诊。在年龄、性别或诊断时的临床特征方面,组间无显著差异。比较BCCH和区域诊所,诱导强尼松暴露(中位数3400,四分位数范围[IQR] 3331-3585 mg/m2 vs 3492, IQR 3397-3644 mg/m2, P = 0.167),年复发率(中位数3.3,IQR 1.1-5.3 vs 2.3, IQR 0.5-4.2, P = 0.575),或频繁复发病程的发展(50% vs 62%, P = 0.475)无差异。第一年的就诊次数(4.2±1.2 vs 4.0±1.8,P = 0.655)和营养师评价的饮食记录(67% vs 47%, P = 0.135, BCCH vs地区)相似。更多的儿童在BCCH接受推荐的眼科监测访问(87% vs 59%, P = 0.01, BCCH vs地区)。局限性:研究的局限性包括样本量小,排除了患有复杂NS的儿童(即诱导期间复发,类固醇抵抗)。结论:自我们实施CNSCP以来,患有NS的儿童在BCCH和区域诊所获得了相当的护理和相似的结果,没有明显的实践差异。
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


