Sushma Agrawal, Rahul, Mohammed Naved Alam, Neeraj Rastogi, Ashish Singh, Rajneesh Kumar Singh, Anu Behari, Prabhakar Mishra
{"title":"Propensity score analysis of adjuvant therapy in radically resected gallbladder cancers: A real world experience from a regional cancer center.","authors":"Sushma Agrawal, Rahul, Mohammed Naved Alam, Neeraj Rastogi, Ashish Singh, Rajneesh Kumar Singh, Anu Behari, Prabhakar Mishra","doi":"10.14701/ahbps.24-169","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Given the high mortality associated with gallbladder cancer (GBC), the efficacy of adjuvant therapy (AT) remains controversial. We audited our data over an 11-year period to assess the impact of AT.</p><p><strong>Methods: </strong>This study included all patients who underwent curative resection for GBC from 2007 to 2017. Analyses were conducted of clinicopathological characteristics, surgical details, and postoperative therapeutic records. The benefits of adjuvant chemotherapy (CT) or chemoradiotherapy (CTRT) were evaluated against surgery alone using SPSS version 20 for statistical analysis.</p><p><strong>Results: </strong>The median age of patients (n = 142) was 50 years. The median overall survival (OS) was 93, 34, and 30 months with CT, CTRT, and surgery alone respectively (<i>p</i> = 0.612). Multivariate analysis indicated that only disease stage and microscopically involved margins significantly impacted OS and disease-free survival (DFS). CT showed increased effectiveness across all prognostic subsets, except for stage 4 and margin-positive resections. Following propensity score matching, median DFS and OS were higher in the CT group than in the CTRT group, although the differences were not statistically significant (<i>p</i> > 0.05).</p><p><strong>Conclusions: </strong>Radically resected GBC patients appear to benefit more from adjuvant CT, while CTRT should be reserved for cases with high-risk features.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"38-47"},"PeriodicalIF":1.7000,"publicationDate":"2025-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11830902/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.24-169","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Backgrounds/aims: Given the high mortality associated with gallbladder cancer (GBC), the efficacy of adjuvant therapy (AT) remains controversial. We audited our data over an 11-year period to assess the impact of AT.
Methods: This study included all patients who underwent curative resection for GBC from 2007 to 2017. Analyses were conducted of clinicopathological characteristics, surgical details, and postoperative therapeutic records. The benefits of adjuvant chemotherapy (CT) or chemoradiotherapy (CTRT) were evaluated against surgery alone using SPSS version 20 for statistical analysis.
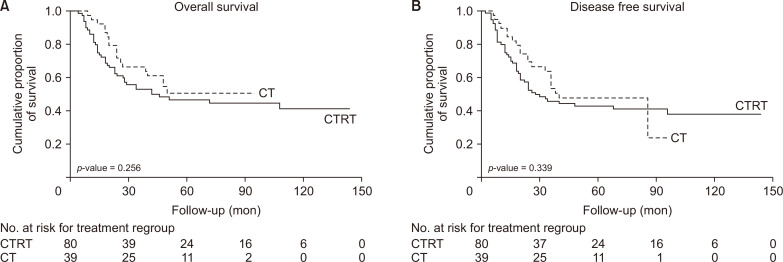
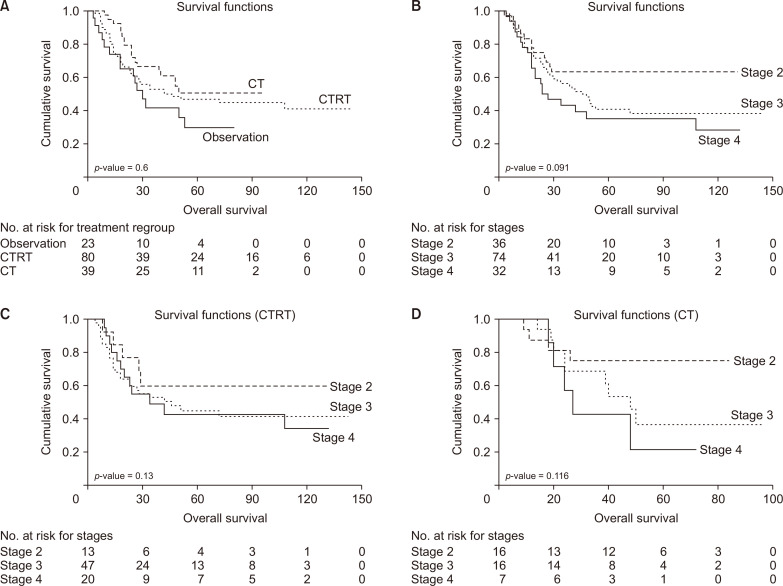
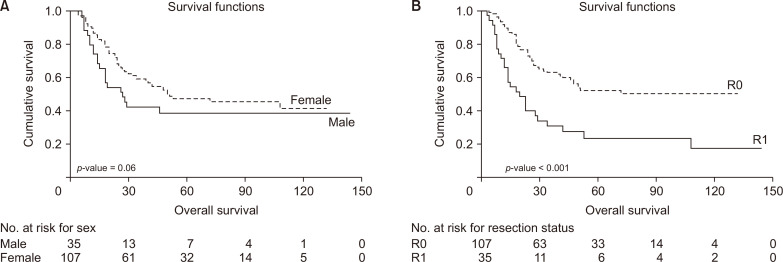
Results: The median age of patients (n = 142) was 50 years. The median overall survival (OS) was 93, 34, and 30 months with CT, CTRT, and surgery alone respectively (p = 0.612). Multivariate analysis indicated that only disease stage and microscopically involved margins significantly impacted OS and disease-free survival (DFS). CT showed increased effectiveness across all prognostic subsets, except for stage 4 and margin-positive resections. Following propensity score matching, median DFS and OS were higher in the CT group than in the CTRT group, although the differences were not statistically significant (p > 0.05).
Conclusions: Radically resected GBC patients appear to benefit more from adjuvant CT, while CTRT should be reserved for cases with high-risk features.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


