Cameron Giles, Karel Huard, André Denault, William Beaubien-Souligny
{"title":"Prediction of Acute Kidney Injury After Cardiac Surgery With Combined Arterial and Venous Intrarenal Doppler.","authors":"Cameron Giles, Karel Huard, André Denault, William Beaubien-Souligny","doi":"10.1177/20543581241309976","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) occurs in up to 50% of cardiac surgical patients and is often hemodynamically mediated. Point-of-care ultrasound is a non-invasive tool that has the potential to characterize intrarenal hemodynamics and predict the risk of AKI.</p><p><strong>Objectives: </strong>We aimed to determine the predictive characteristics of intrarenal arterial and venous Doppler markers for postoperative AKI in cardiac surgical patients.</p><p><strong>Design: </strong>This study is the secondary analysis of a prospective cohort study.</p><p><strong>Setting: </strong>This study is carried out in a care academic cardiac surgical center in Montreal, Quebec, Canada.</p><p><strong>Patients: </strong>Adult patients undergoing cardiac surgery with the use of cardiopulmonary bypass.</p><p><strong>Measurements: </strong>Point-of-care ultrasound assessments were performed preoperatively and at intensive care unit admission. Arterial measurements included the renal resistive index (RRI) and intrarenal artery velocity-time integral normalized to peak systolic velocity (VTI/PSV). Venous measurements included intrarenal venous flow (IRVF) pattern and renal venous stasis index (RVSI).</p><p><strong>Methods: </strong>We used area under the receiving operating characteristic curves (AUCs) with net reclassification index (NRI) and multivariable logistic regression to determine predictive characteristics for postoperative AKI. Furthermore, we used hierarchical clustering to identify potential groups with similar Doppler parameters and performed comparisons of patients' characteristics and outcomes between groups.</p><p><strong>Results: </strong>We included 136 patients with 47 (34.6%) developing postoperative AKI. At intensive care unit admission, arterial indices showed similar discrimination for the prediction of AKI (RRI: AUC = 0.64; 95% confidence interval (CI) = 0.55 to 0.74; and VTI/PSV: AUC = 0.67; 95% CI = 0.57 to 0.77). Venous Doppler indices including IRVF patterns (AUC = 0.64; 95% CI = 0.53 to 0.74) and RVSI (AUC = 0.60; 95% CI = 0.50 to 0.71) also showed similar performance. The combined model of RRI and IRVF pattern (AUC = 0.69; 95% CI = 0.59 to 0.78) improved the prediction of AKI compared to either RRI (NRI = 0.50; 95% CI = 0.17 to 0.84) or IRVF pattern (NRI = 0.38; 95% CI = 0.04 to 0.70) alone. Through hierarchical clustering, we identified 3 groups (1: low RRI, 2: high RRI/low RVSI, and 3: high RRI/high RVSI) with different patient characteristics and outcomes. The patient in group 3 had a higher risk of AKI and worse clinical outcomes compared with other groups.</p><p><strong>Limitations: </strong>Single-center design in cardiac surgical patients limits generalizability.</p><p><strong>Conclusions: </strong>Although more complex indices of intrarenal Doppler indices including the VTI/PSV and RVSI did not improve prediction of postoperative AKI, combining RRI and IRVF pattern improved risk prediction for AKI. Intrarenal arteriovenous Doppler subphenotypes identified patient groups at high risk of postoperative AKI.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241309976"},"PeriodicalIF":1.5000,"publicationDate":"2024-12-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11672484/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241309976","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute kidney injury (AKI) occurs in up to 50% of cardiac surgical patients and is often hemodynamically mediated. Point-of-care ultrasound is a non-invasive tool that has the potential to characterize intrarenal hemodynamics and predict the risk of AKI.
Objectives: We aimed to determine the predictive characteristics of intrarenal arterial and venous Doppler markers for postoperative AKI in cardiac surgical patients.
Design: This study is the secondary analysis of a prospective cohort study.
Setting: This study is carried out in a care academic cardiac surgical center in Montreal, Quebec, Canada.
Patients: Adult patients undergoing cardiac surgery with the use of cardiopulmonary bypass.
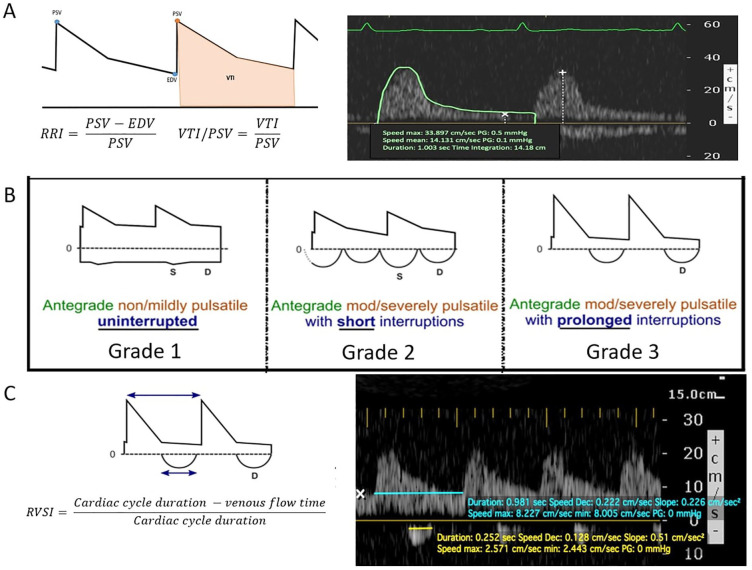
Measurements: Point-of-care ultrasound assessments were performed preoperatively and at intensive care unit admission. Arterial measurements included the renal resistive index (RRI) and intrarenal artery velocity-time integral normalized to peak systolic velocity (VTI/PSV). Venous measurements included intrarenal venous flow (IRVF) pattern and renal venous stasis index (RVSI).
Methods: We used area under the receiving operating characteristic curves (AUCs) with net reclassification index (NRI) and multivariable logistic regression to determine predictive characteristics for postoperative AKI. Furthermore, we used hierarchical clustering to identify potential groups with similar Doppler parameters and performed comparisons of patients' characteristics and outcomes between groups.
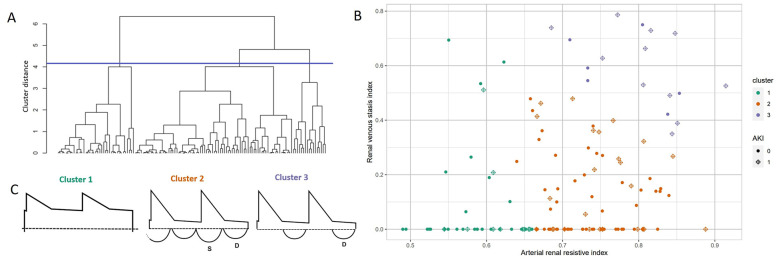
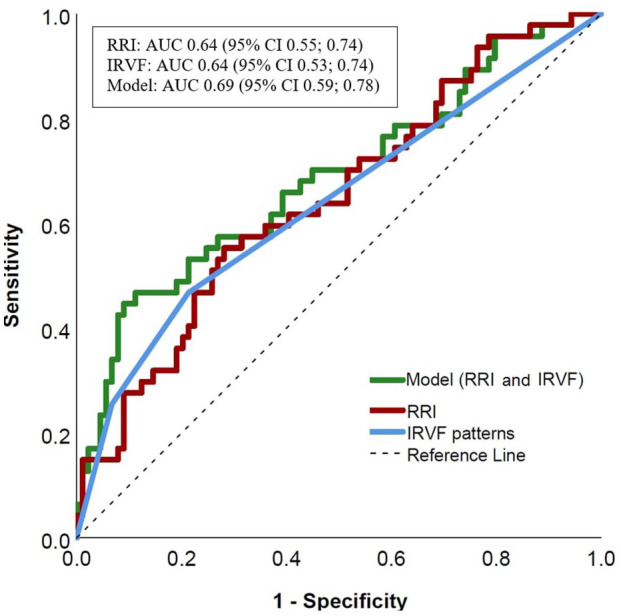
Results: We included 136 patients with 47 (34.6%) developing postoperative AKI. At intensive care unit admission, arterial indices showed similar discrimination for the prediction of AKI (RRI: AUC = 0.64; 95% confidence interval (CI) = 0.55 to 0.74; and VTI/PSV: AUC = 0.67; 95% CI = 0.57 to 0.77). Venous Doppler indices including IRVF patterns (AUC = 0.64; 95% CI = 0.53 to 0.74) and RVSI (AUC = 0.60; 95% CI = 0.50 to 0.71) also showed similar performance. The combined model of RRI and IRVF pattern (AUC = 0.69; 95% CI = 0.59 to 0.78) improved the prediction of AKI compared to either RRI (NRI = 0.50; 95% CI = 0.17 to 0.84) or IRVF pattern (NRI = 0.38; 95% CI = 0.04 to 0.70) alone. Through hierarchical clustering, we identified 3 groups (1: low RRI, 2: high RRI/low RVSI, and 3: high RRI/high RVSI) with different patient characteristics and outcomes. The patient in group 3 had a higher risk of AKI and worse clinical outcomes compared with other groups.
Limitations: Single-center design in cardiac surgical patients limits generalizability.
Conclusions: Although more complex indices of intrarenal Doppler indices including the VTI/PSV and RVSI did not improve prediction of postoperative AKI, combining RRI and IRVF pattern improved risk prediction for AKI. Intrarenal arteriovenous Doppler subphenotypes identified patient groups at high risk of postoperative AKI.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


