Development of Nonketotic Hyperglycemia Requiring High-Dose Insulin After Supratherapeutic Amlodipine Ingestion
IF 1.2
Q3 Medicine
引用次数: 0
Abstract
Background/Objective
Calcium channel blockers, when taken in overdose quantities, can cause hyperglycemia requiring so-called hyperinsulinemic-euglycemic therapy. The objective of this report was to describe a patient with calcium channel blocker toxicity resulting from overdose of amlodipine.
Case Report
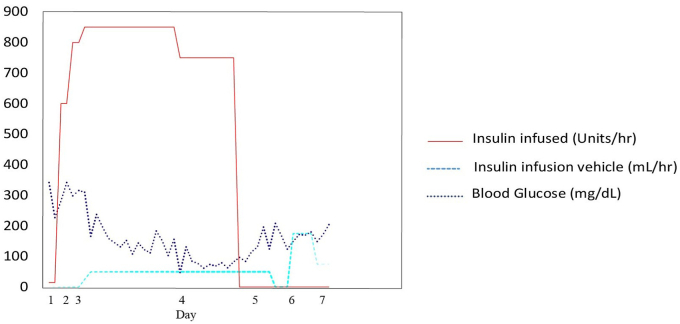
A 74-year-old man presented with a fall and loss of consciousness. Prior to this event, he consumed 88 tablets of amlodipine. Medical history was significant for hypertension, hyperlipidemia, and cerebrovascular accident. His vital signs were heart rate of 51 beats/min, blood pressure of 162/137 mm Hg, oxygen saturation of 94% on room air, and respiratory rate of 16 breaths/min. The patient soon became hypotensive. The blood glucose level was 227 mg/dL. Urinalysis was negative for ketones. The patient was diagnosed with calcium channel blocker toxicity and admitted to the intensive care unit. He received continuous insulin infusion and dextrose 25% in water for 5 and 7 days respectively, with a peak insulin infusion rate of 850 U/h. After discontinuation of medications, the glucose level, blood pressure, and heart rate were 82 mg/dL, 127/68 mm Hg, and 86 beats/min, respectively, and he returned to prior functional status.
Discussion
Amlodipine is a long-acting dihydropyridine class calcium channel blocking drug. In the overdose setting, amlodipine inhibits calcium uptake by myocytes and release of insulin from pancreatic beta cells.
Conclusion
In this case, high-dose insulin euglycemic therapy was effective in the treatment of amlodipine overdose and should be considered in similar cases.
超治疗性氨氯地平摄入后需要大剂量胰岛素的非酮症高血糖的发展。
背景/目的:过量服用钙通道阻滞剂可引起高血糖,需要所谓的高胰岛素-降糖治疗。本报告的目的是描述一个病人钙通道阻滞剂毒性导致过量氨氯地平。病例报告:一名74岁男性,表现为跌倒和意识丧失。在此之前,他服用了88片氨氯地平。有高血压、高脂血症及脑血管意外病史。生命体征:心率51次/分,血压162/137毫米汞柱,室内空气氧饱和度94%,呼吸频率16次/分。病人很快出现低血压。血糖227毫克/分升。尿检酮类呈阴性。患者被诊断为钙通道阻滞剂毒性,并住进重症监护室。连续输注胰岛素和25%水葡萄糖,分别5天和7天,胰岛素输注速率峰值为850 U/h。停药后,血糖、血压和心率分别为82 mg/dL、127/68 mm Hg和86次/分,恢复到之前的功能状态。讨论:氨氯地平是一种长效二氢吡啶类钙通道阻断药物。在过量的情况下,氨氯地平抑制心肌细胞对钙的摄取和胰腺β细胞对胰岛素的释放。结论:本病例采用高剂量胰岛素正糖治疗氨氯地平过量是有效的,在类似病例中应予以考虑。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

AACE Clinical Case Reports
Medicine-Endocrinology, Diabetes and Metabolism
CiteScore
2.30
自引率
0.00%
发文量
61
审稿时长
55 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


