Andrew A Lawson, Kae Watanabe, Lindsay Griffin, Christina Laternser, Michael Markl, Cynthia K Rigsby, Joshua D Robinson, Nazia Husain
{"title":"Multiparametric cardiovascular magnetic resonance is associated with outcomes in pediatric heart transplant recipients.","authors":"Andrew A Lawson, Kae Watanabe, Lindsay Griffin, Christina Laternser, Michael Markl, Cynthia K Rigsby, Joshua D Robinson, Nazia Husain","doi":"10.1016/j.jocmr.2024.101138","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multiparametric cardiovascular magnetic resonance (CMR) has an emerging role in non-invasive surveillance of pediatric heart transplant recipients (PHTR). Higher myocardial T2, higher extracellular volume fraction (ECV), and late gadolinium enhancement (LGE) have been associated with adverse clinical outcomes in adult heart transplant recipients. The purpose of this study was to investigate the prognostic value of CMR-derived T1 and T2 mapping, ECV, and LGE for clinical outcomes in PHTR.</p><p><strong>Methods: </strong>We performed a single-center, retrospective chart review of consecutive, gadolinium-enhanced CMR studies in PHTR over a 7.5-year period, excluding follow-up studies. Standard CMR ventricular volume and function analysis, T1 mapping with ECV, T2 mapping, and LGE assessment were performed. The composite outcome included cardiac death, non-cardiac death, re-transplantation, and cardiac hospitalization.</p><p><strong>Results: </strong>Among 113 PHTR, mean age was 13.0 ± 5.1 years, with 6.0 ± 4.0 years since transplant. The indication for CMR was surveillance in 79%. Mean native T1 was 1050 ± 48 ms, T2 49.2 ± 3.9 ms, and ECV 29.7 ± 4.5%. Left ventricular LGE was present in 37% (42/113) and right ventricular LGE in 3.5% (4/113). The mean follow-up time was 2.3 years and median was 1.4 years. Cardiac death occurred in 2% (2/113), re-transplantation in 4% (4/113), and cardiac hospitalization in 22% (25/113). Non-cardiac death did not occur. Using Kaplan-Meier analysis, high T1 (≥1061 ms), T2 (≥50.0 ms), and ECV (≥31.4%) were each associated with decreased freedom from the composite outcome in follow-up. In univariable Cox regression analyses, high T1 was associated with increased risk of the composite outcome (hazard ratios [HR] 4.0, 95% confidence interval [CI] 1.7-9.2, p = 0.001), as were high T2 (HR 2.8, 95% CI 1.1-7.1, p = 0.026), and high ECV (HR 3.5, 95% CI 1.5-8.1, p = 0.004).</p><p><strong>Conclusion: </strong>T1 and T2 mapping are associated with early differences in adverse cardiac events in PHTR. These data suggest a role for a multicenter study with a longer follow-up duration.</p>","PeriodicalId":15221,"journal":{"name":"Journal of Cardiovascular Magnetic Resonance","volume":" ","pages":"101138"},"PeriodicalIF":6.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11783449/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Magnetic Resonance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jocmr.2024.101138","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/25 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Multiparametric cardiovascular magnetic resonance (CMR) has an emerging role in non-invasive surveillance of pediatric heart transplant recipients (PHTR). Higher myocardial T2, higher extracellular volume fraction (ECV), and late gadolinium enhancement (LGE) have been associated with adverse clinical outcomes in adult heart transplant recipients. The purpose of this study was to investigate the prognostic value of CMR-derived T1 and T2 mapping, ECV, and LGE for clinical outcomes in PHTR.
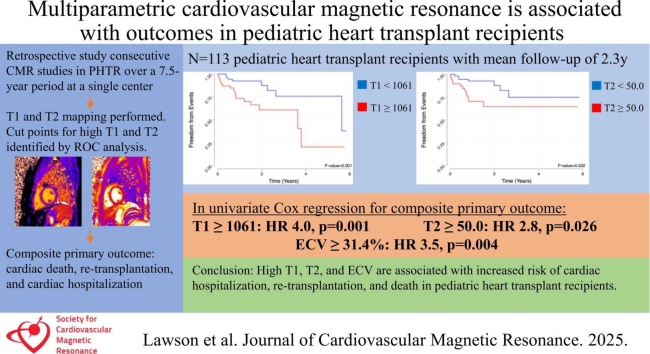
Methods: We performed a single-center, retrospective chart review of consecutive, gadolinium-enhanced CMR studies in PHTR over a 7.5-year period, excluding follow-up studies. Standard CMR ventricular volume and function analysis, T1 mapping with ECV, T2 mapping, and LGE assessment were performed. The composite outcome included cardiac death, non-cardiac death, re-transplantation, and cardiac hospitalization.
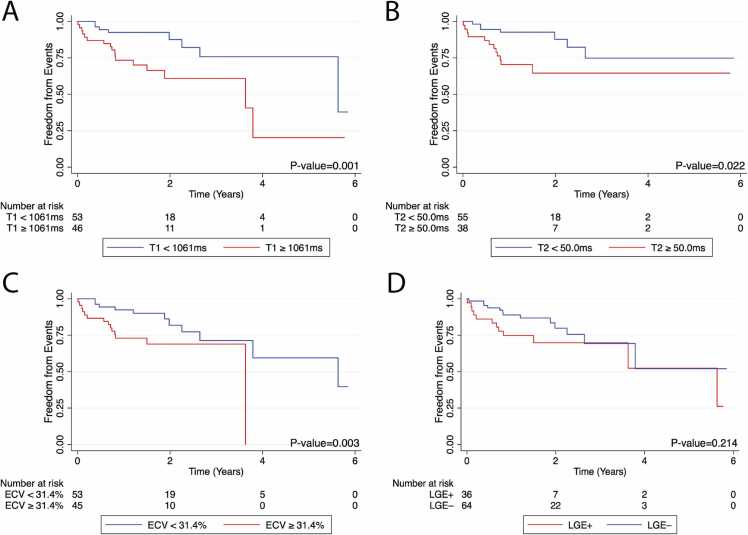
Results: Among 113 PHTR, mean age was 13.0 ± 5.1 years, with 6.0 ± 4.0 years since transplant. The indication for CMR was surveillance in 79%. Mean native T1 was 1050 ± 48 ms, T2 49.2 ± 3.9 ms, and ECV 29.7 ± 4.5%. Left ventricular LGE was present in 37% (42/113) and right ventricular LGE in 3.5% (4/113). The mean follow-up time was 2.3 years and median was 1.4 years. Cardiac death occurred in 2% (2/113), re-transplantation in 4% (4/113), and cardiac hospitalization in 22% (25/113). Non-cardiac death did not occur. Using Kaplan-Meier analysis, high T1 (≥1061 ms), T2 (≥50.0 ms), and ECV (≥31.4%) were each associated with decreased freedom from the composite outcome in follow-up. In univariable Cox regression analyses, high T1 was associated with increased risk of the composite outcome (hazard ratios [HR] 4.0, 95% confidence interval [CI] 1.7-9.2, p = 0.001), as were high T2 (HR 2.8, 95% CI 1.1-7.1, p = 0.026), and high ECV (HR 3.5, 95% CI 1.5-8.1, p = 0.004).
Conclusion: T1 and T2 mapping are associated with early differences in adverse cardiac events in PHTR. These data suggest a role for a multicenter study with a longer follow-up duration.
期刊介绍:
Journal of Cardiovascular Magnetic Resonance (JCMR) publishes high-quality articles on all aspects of basic, translational and clinical research on the design, development, manufacture, and evaluation of cardiovascular magnetic resonance (CMR) methods applied to the cardiovascular system. Topical areas include, but are not limited to:
New applications of magnetic resonance to improve the diagnostic strategies, risk stratification, characterization and management of diseases affecting the cardiovascular system.
New methods to enhance or accelerate image acquisition and data analysis.
Results of multicenter, or larger single-center studies that provide insight into the utility of CMR.
Basic biological perceptions derived by CMR methods.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


