Indications, complications and outcomes of minimally-invasive lateral lumbar interbody fusion with anterior column realignment vs. standard LLIF using expandable interbody spacers.
Gregor Fischer, Linda Bättig, Thomas Schöfl, Ethan Schonfeld, Anand Veeravagu, Benjamin Martens, Martin N Stienen
{"title":"Indications, complications and outcomes of minimally-invasive lateral lumbar interbody fusion with anterior column realignment vs. standard LLIF using expandable interbody spacers.","authors":"Gregor Fischer, Linda Bättig, Thomas Schöfl, Ethan Schonfeld, Anand Veeravagu, Benjamin Martens, Martin N Stienen","doi":"10.3389/fsurg.2024.1455445","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anterior column realignment (ACR), using a lateral lumbar or thoracic interbody fusion (LLIF) approach to release the anterior longitudinal ligament (ALL), is a powerful technique to increase segmental lordosis. We here report our experience with the use of expandible LLIF cages for ACR.</p><p><strong>Methods: </strong>Retrospective, single-center observational cohort study including consecutive patients treated by LLIF using an expandible interbody implant. Patients with ACR were compared to patients without ACR. Our outcomes include adverse events (AEs), radiological (segmental sagittal cobb angle, spinopelvic parameters) and clinical outcomes until 12 months postoperative.</p><p><strong>Results: </strong>We identified 503 patients, in which we performed LLIF at 732 levels. In 63 patients (12.5%) and 70 levels (9.6%) an expandable cage was used. Of those, in 30 patients (47.6%) and 30 levels, the ALL was released (42.8%). Age (mean 61.4 years), sex (57.1% female), comorbidities and further demographic features were similar, but patients in the ACR group had a higher anesthesiologic risk, were more frequently operated for degenerative deformity and had a more severely dysbalanced spine (all <i>p</i> < 0.05). ACR was most frequently done at L3/4 (36.7%) and L4/5 (23.3%), entailing multilevel fusions in 50% (3-7 levels) and long constructs in 26.7% (>7 levels). Intraoperative AEs occurred in 3.3% (ACR) and 3.0% (no ACR; <i>p</i> = 0.945). In ACR cases, mean segmental lordosis changed from -2.8° (preoperative) to 16.4° (discharge; <i>p</i> < 0.001), 15.0° (3 months; <i>p</i> < 0.001) and 16.9° (12 months; <i>p</i> < 0.001), whereas this change was less in non-ACR cases [4.3° vs. 10.5° (discharge; <i>p</i> < 0.05), 10.9 (3 months; <i>p</i> < 0.05) and 10.4 (12 months; <i>p</i> > 0.05)]. Total lumbar lordosis increased from 27.8° to 45.2° (discharge; <i>p</i> < 0.001), 45.8° (3 months; <i>p</i> < 0.001) and 41.9° (12 months; <i>p</i> < 0.001) in ACR cases and from 37.4° to 46.7° (discharge; <i>p</i> < 0.01), 44.6° (3 months; n.s.) and 44.9° (12 months; n.s.) in non-ACR cases. Rates of AEs and clinical outcomes at 3 and 12 months were similar (all <i>p</i> > 0.05) and no pseudarthrosis at the LLIF level was noted.</p><p><strong>Conclusions: </strong>ACR using an expandible LLIF interbody implant was safe, promoted solid fusion and restored significantly more segmental lordosis compared to LLIF without ALL release, which was maintained during follow-up.</p>","PeriodicalId":12564,"journal":{"name":"Frontiers in Surgery","volume":"11 ","pages":"1455445"},"PeriodicalIF":1.6000,"publicationDate":"2024-12-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11663892/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fsurg.2024.1455445","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Anterior column realignment (ACR), using a lateral lumbar or thoracic interbody fusion (LLIF) approach to release the anterior longitudinal ligament (ALL), is a powerful technique to increase segmental lordosis. We here report our experience with the use of expandible LLIF cages for ACR.
Methods: Retrospective, single-center observational cohort study including consecutive patients treated by LLIF using an expandible interbody implant. Patients with ACR were compared to patients without ACR. Our outcomes include adverse events (AEs), radiological (segmental sagittal cobb angle, spinopelvic parameters) and clinical outcomes until 12 months postoperative.
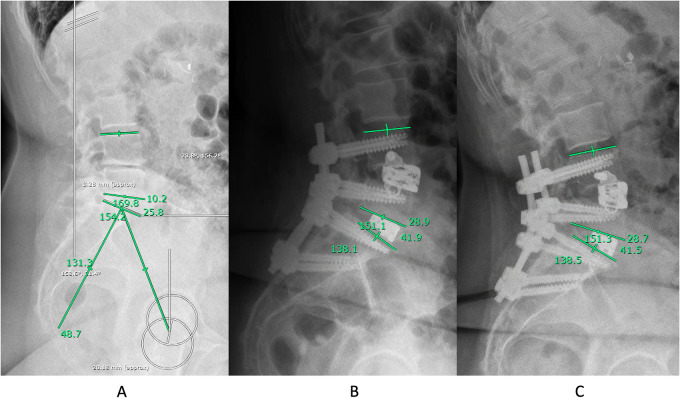
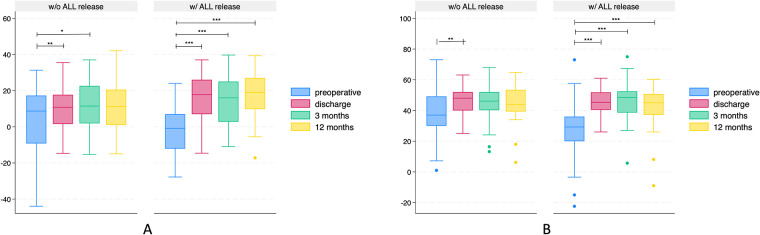
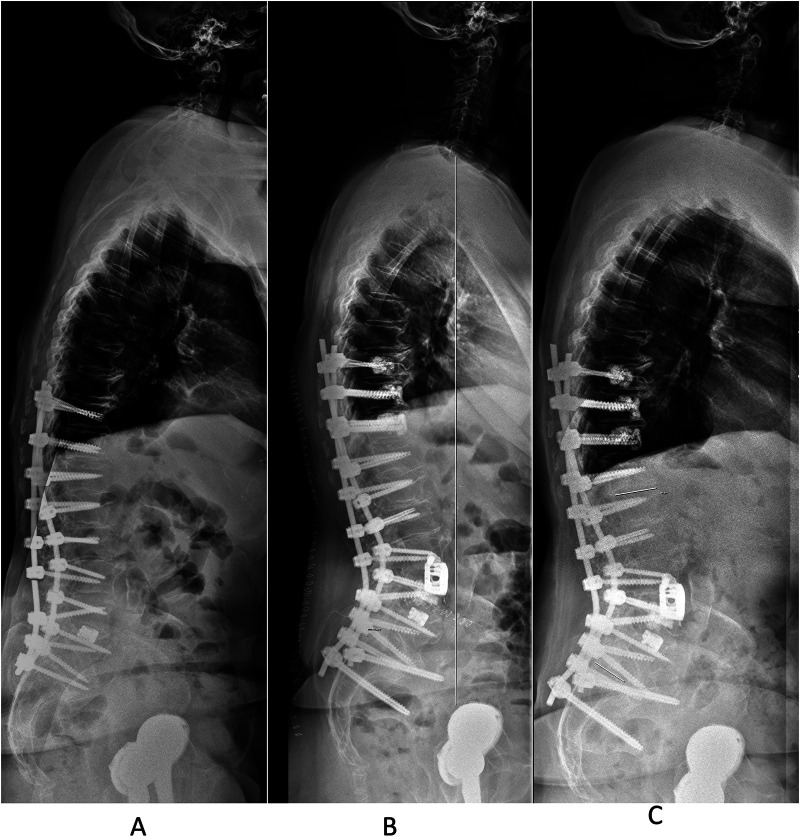
Results: We identified 503 patients, in which we performed LLIF at 732 levels. In 63 patients (12.5%) and 70 levels (9.6%) an expandable cage was used. Of those, in 30 patients (47.6%) and 30 levels, the ALL was released (42.8%). Age (mean 61.4 years), sex (57.1% female), comorbidities and further demographic features were similar, but patients in the ACR group had a higher anesthesiologic risk, were more frequently operated for degenerative deformity and had a more severely dysbalanced spine (all p < 0.05). ACR was most frequently done at L3/4 (36.7%) and L4/5 (23.3%), entailing multilevel fusions in 50% (3-7 levels) and long constructs in 26.7% (>7 levels). Intraoperative AEs occurred in 3.3% (ACR) and 3.0% (no ACR; p = 0.945). In ACR cases, mean segmental lordosis changed from -2.8° (preoperative) to 16.4° (discharge; p < 0.001), 15.0° (3 months; p < 0.001) and 16.9° (12 months; p < 0.001), whereas this change was less in non-ACR cases [4.3° vs. 10.5° (discharge; p < 0.05), 10.9 (3 months; p < 0.05) and 10.4 (12 months; p > 0.05)]. Total lumbar lordosis increased from 27.8° to 45.2° (discharge; p < 0.001), 45.8° (3 months; p < 0.001) and 41.9° (12 months; p < 0.001) in ACR cases and from 37.4° to 46.7° (discharge; p < 0.01), 44.6° (3 months; n.s.) and 44.9° (12 months; n.s.) in non-ACR cases. Rates of AEs and clinical outcomes at 3 and 12 months were similar (all p > 0.05) and no pseudarthrosis at the LLIF level was noted.
Conclusions: ACR using an expandible LLIF interbody implant was safe, promoted solid fusion and restored significantly more segmental lordosis compared to LLIF without ALL release, which was maintained during follow-up.
背景:采用侧位腰椎或胸椎体间融合(LLIF)入路释放前纵韧带(ALL)的前柱重组(ACR)是增加节段性前凸的有力技术。我们在此报告我们在ACR中使用可扩展lliff笼的经验。方法:回顾性,单中心观察队列研究,包括使用可扩展体间植入物进行LLIF治疗的连续患者。将有ACR的患者与无ACR的患者进行比较。我们的结果包括不良事件(ae)、放射学(节段矢状cobb角、脊柱骨盆参数)和临床结果,直到术后12个月。结果:我们确定了503例患者,其中我们在732个水平上进行了LLIF。63例患者(12.5%)和70个水平(9.6%)使用了可膨胀笼。其中,30名患者(47.6%)和30个水平的ALL被释放(42.8%)。年龄(平均61.4岁)、性别(57.1%为女性)、合并症和进一步的人口学特征相似,但ACR组患者有更高的麻醉风险,更频繁地因退行性畸形手术,脊柱失衡更严重(均为p7水平)。术中不良事件发生率分别为3.3%(无ACR)和3.0%(无ACR);p = 0.945)。在ACR病例中,平均节段性前凸从术前的-2.8°变化到出院时的16.4°;p p p p p > 0.05)]。腰椎前凸度从27.8°增加到45.2°(出院;p p p p > 0.05), LLIF水平未见假关节。结论:与未释放ALL的LLIF相比,使用可扩展LLIF椎体间种植体的ACR是安全的,促进了固体融合,并明显恢复了更多的节段性前凸,并在随访期间保持。
期刊介绍:
Evidence of surgical interventions go back to prehistoric times. Since then, the field of surgery has developed into a complex array of specialties and procedures, particularly with the advent of microsurgery, lasers and minimally invasive techniques. The advanced skills now required from surgeons has led to ever increasing specialization, though these still share important fundamental principles.
Frontiers in Surgery is the umbrella journal representing the publication interests of all surgical specialties. It is divided into several “Specialty Sections” listed below. All these sections have their own Specialty Chief Editor, Editorial Board and homepage, but all articles carry the citation Frontiers in Surgery.
Frontiers in Surgery calls upon medical professionals and scientists from all surgical specialties to publish their experimental and clinical studies in this journal. By assembling all surgical specialties, which nonetheless retain their independence, under the common umbrella of Frontiers in Surgery, a powerful publication venue is created. Since there is often overlap and common ground between the different surgical specialties, assembly of all surgical disciplines into a single journal will foster a collaborative dialogue amongst the surgical community. This means that publications, which are also of interest to other surgical specialties, will reach a wider audience and have greater impact.
The aim of this multidisciplinary journal is to create a discussion and knowledge platform of advances and research findings in surgical practice today to continuously improve clinical management of patients and foster innovation in this field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


