Laparoscopic-assisted versus ultrasound-guided transversus abdominis plane block for laparoscopic cholecystectomy: a systematic review and meta-analysis.
Sundus Abdul Ghani, Hassan Ul Hussain, Maryam Abdul Wahid, Neha Majeed, Sheeba Burney, Areesha Tanveer, Muhammad Sohaib Asghar
{"title":"Laparoscopic-assisted versus ultrasound-guided transversus abdominis plane block for laparoscopic cholecystectomy: a systematic review and meta-analysis.","authors":"Sundus Abdul Ghani, Hassan Ul Hussain, Maryam Abdul Wahid, Neha Majeed, Sheeba Burney, Areesha Tanveer, Muhammad Sohaib Asghar","doi":"10.1186/s12893-024-02706-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Laparoscopic-assisted (LTAP) and ultrasound-guided (UTAP) transversus abdominis plane (TAP) blocks are widely used for postoperative analgesia in laparoscopic cholecystectomy (LC), yet their comparative effectiveness remains unclear. The aim of this meta-analysis was to systematically evaluate and compare postoperative outcomes of LTAP and UTAP in LC.</p><p><strong>Materials and methodology: </strong>A comprehensive literature search of five electronic databases was conducted from the inception of the paper till 2 June 2024 following PRISMA guidelines. Eligibility criteria included: (a) randomized controlled trials (RCTs); (b) adult patients (≥ 18 years) undergoing elective LC; (c) intervention group undergoing LTAP; (d) control group receiving UTAP; (e) outcomes: postoperative pain intensity using VAS score; time to first analgesic need; postoperative morphine consumption; postoperative nausea vomiting (PONV); time to first bowel evacuation; time to first flatus. Mendeley Desktop 1.19.8 was used for article retrieval and for the removal of duplicates. Risk of bias was assessed using the Cochrane Risk of Bias Tool, and statistical analysis was performed using Review Manager, applying a random-effects model. Forest plots represented combined effects of Risk Ratios (RRs) for dichotomous outcomes and weighted mean differences (WMDs) for continuous outcomes with a 95% confidence interval (CI). P-value ≤ 0.05 was considered statistically significant and Higgin's I² test was employed to assess heterogeneity.</p><p><strong>Results: </strong>Seven RCTs in total involving 603 patients were included in the analysis, with 236 patients in the LTAP group and 232 in the UTAP group. No statistically significant differences observed between LTAP and UTAP in postoperative pain intensity at 6, 12, and 24 h, time to first analgesic need, postoperative morphine consumption, PONV, time to first stools, and time to first flatus, initially. Sensitivity analysis revealed a significant reduction in 6-hour postoperative pain in the LTAP group (WMD = 0.39; 95% CI = 0.10,0.67; P = 0.008; I² = 0%), but no significant differences were found in later time points (12 h: WMD = 0.12; 95% CI = -0.17,0.40; P = 0.42; I² = 0%; 24 h: WMD = -0.04; 95% CI = -0.26, 0.18; P = 0.73; I² = 5%) or in other outcomes. Moderate levels of heterogeneity and an overall low risk of bias in quality assessment were observed among the studies.</p><p><strong>Conclusion: </strong>Our meta-analysis indicated no clear advantage of LTAP over UTAP in managing postoperative pain and related outcomes in LC. Although LTAP may offer logistical benefits by reducing the need for equipment and personnel, further large-scale RCTs focusing on procedure-specific outcomes are needed to establish definitive conclusions.</p>","PeriodicalId":49229,"journal":{"name":"BMC Surgery","volume":"24 1","pages":"400"},"PeriodicalIF":1.8000,"publicationDate":"2024-12-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11662483/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12893-024-02706-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Laparoscopic-assisted (LTAP) and ultrasound-guided (UTAP) transversus abdominis plane (TAP) blocks are widely used for postoperative analgesia in laparoscopic cholecystectomy (LC), yet their comparative effectiveness remains unclear. The aim of this meta-analysis was to systematically evaluate and compare postoperative outcomes of LTAP and UTAP in LC.
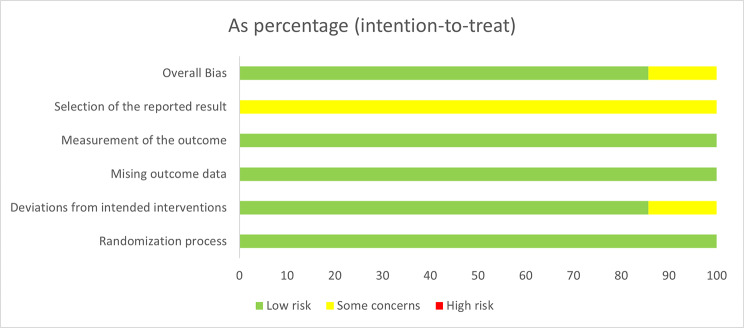
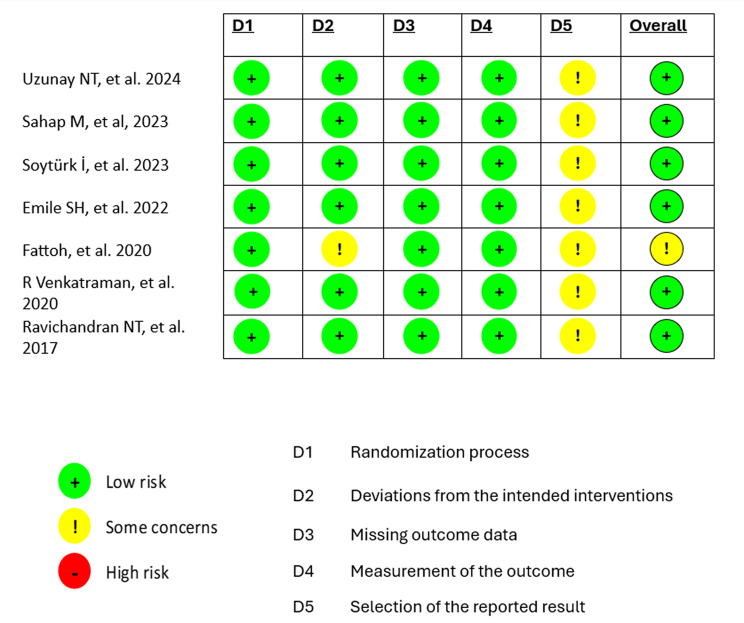
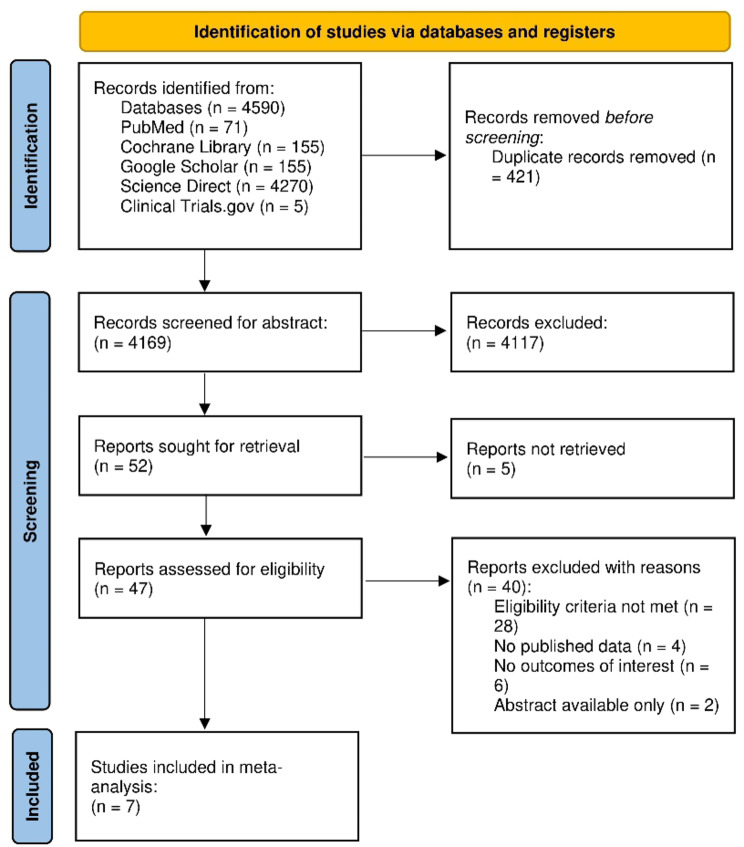
Materials and methodology: A comprehensive literature search of five electronic databases was conducted from the inception of the paper till 2 June 2024 following PRISMA guidelines. Eligibility criteria included: (a) randomized controlled trials (RCTs); (b) adult patients (≥ 18 years) undergoing elective LC; (c) intervention group undergoing LTAP; (d) control group receiving UTAP; (e) outcomes: postoperative pain intensity using VAS score; time to first analgesic need; postoperative morphine consumption; postoperative nausea vomiting (PONV); time to first bowel evacuation; time to first flatus. Mendeley Desktop 1.19.8 was used for article retrieval and for the removal of duplicates. Risk of bias was assessed using the Cochrane Risk of Bias Tool, and statistical analysis was performed using Review Manager, applying a random-effects model. Forest plots represented combined effects of Risk Ratios (RRs) for dichotomous outcomes and weighted mean differences (WMDs) for continuous outcomes with a 95% confidence interval (CI). P-value ≤ 0.05 was considered statistically significant and Higgin's I² test was employed to assess heterogeneity.
Results: Seven RCTs in total involving 603 patients were included in the analysis, with 236 patients in the LTAP group and 232 in the UTAP group. No statistically significant differences observed between LTAP and UTAP in postoperative pain intensity at 6, 12, and 24 h, time to first analgesic need, postoperative morphine consumption, PONV, time to first stools, and time to first flatus, initially. Sensitivity analysis revealed a significant reduction in 6-hour postoperative pain in the LTAP group (WMD = 0.39; 95% CI = 0.10,0.67; P = 0.008; I² = 0%), but no significant differences were found in later time points (12 h: WMD = 0.12; 95% CI = -0.17,0.40; P = 0.42; I² = 0%; 24 h: WMD = -0.04; 95% CI = -0.26, 0.18; P = 0.73; I² = 5%) or in other outcomes. Moderate levels of heterogeneity and an overall low risk of bias in quality assessment were observed among the studies.
Conclusion: Our meta-analysis indicated no clear advantage of LTAP over UTAP in managing postoperative pain and related outcomes in LC. Although LTAP may offer logistical benefits by reducing the need for equipment and personnel, further large-scale RCTs focusing on procedure-specific outcomes are needed to establish definitive conclusions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


