Maryam Moradi, Ali Talebi, Sara Shavakhi, Mohammad Javad Tarrahi, Fouad Meraji Far
{"title":"Coronary artery calcification score as the determinant of coronary artery disease in chronic kidney disease patients: A preliminary study.","authors":"Maryam Moradi, Ali Talebi, Sara Shavakhi, Mohammad Javad Tarrahi, Fouad Meraji Far","doi":"10.48305/arya.2023.39234.2832","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronary computed tomography angiography (CCTA) is a noninvasive cardiovascular imaging procedure that visualizes coronary artery calcifications (CAC), a marker of subclinical atherosclerosis. Due to different calcification patterns in patients with chronic kidney disease (CKD) compared to the general population, this study aims to present diagnostic cut-off values for CAC to detect early coronary artery disease (CAD) in CKD patients.</p><p><strong>Methods: </strong>This cross-sectional study included 807 patients: 407 with CKD and 400 controls with normal kidney function who underwent CCTA during 2019-2021. CAC score measurements were performed for all left main coronary arteries to investigate CAD. The Coronary Artery Disease Reporting and Data System (CAD-RADS) was used as the gold standard to determine the value of CAC, and diagnostic values were measured.</p><p><strong>Results: </strong>The number of female patients was 443 (54.9%), and 364 (45.1%) were male. The mean age in the case group was 63.95 ± 10.26 years, and in the control group, it was 53.80 ± 11.84 years. At the cut-off point of 85, the CAC score had a sensitivity and specificity of 84.7% and 83%, respectively, among patients with CKD to detect CAD (Area Under the Curve (AUC): 0.919, 95% CI: 0.89-0.94; P-value < 0.001). Considering a cut-point of 85 for CAC, the frequency of healthy subjects with CAD-RADS less than two was significantly higher than the cases (P-value = 0.012), while the two groups were similar regarding CAD-RADS 3-5 (P-value = 0.83).</p><p><strong>Conclusion: </strong>According to this study, the CAC score is a valuable means to detect CAD among CKD subjects. There is no significant difference in CAC between patients with substantial CAD-RADS in CKD and non-CKD patients. The cut-point of 85 for the CAC score was found valuable to diagnose CAD with over 80% sensitivity and specificity.</p>","PeriodicalId":46477,"journal":{"name":"ARYA Atherosclerosis","volume":"20 3","pages":"12-20"},"PeriodicalIF":0.6000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11651311/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ARYA Atherosclerosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.48305/arya.2023.39234.2832","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Coronary computed tomography angiography (CCTA) is a noninvasive cardiovascular imaging procedure that visualizes coronary artery calcifications (CAC), a marker of subclinical atherosclerosis. Due to different calcification patterns in patients with chronic kidney disease (CKD) compared to the general population, this study aims to present diagnostic cut-off values for CAC to detect early coronary artery disease (CAD) in CKD patients.
Methods: This cross-sectional study included 807 patients: 407 with CKD and 400 controls with normal kidney function who underwent CCTA during 2019-2021. CAC score measurements were performed for all left main coronary arteries to investigate CAD. The Coronary Artery Disease Reporting and Data System (CAD-RADS) was used as the gold standard to determine the value of CAC, and diagnostic values were measured.
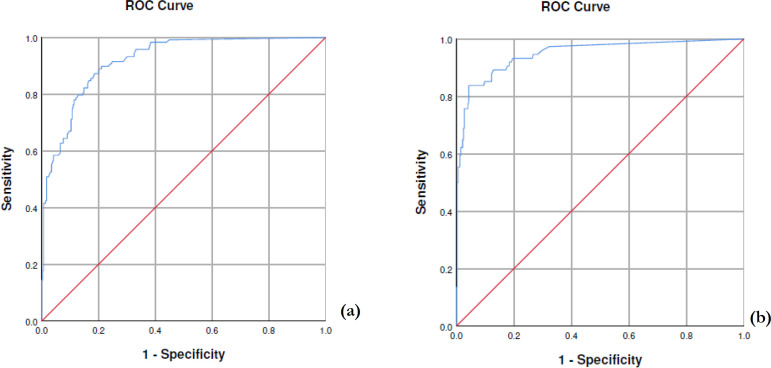
Results: The number of female patients was 443 (54.9%), and 364 (45.1%) were male. The mean age in the case group was 63.95 ± 10.26 years, and in the control group, it was 53.80 ± 11.84 years. At the cut-off point of 85, the CAC score had a sensitivity and specificity of 84.7% and 83%, respectively, among patients with CKD to detect CAD (Area Under the Curve (AUC): 0.919, 95% CI: 0.89-0.94; P-value < 0.001). Considering a cut-point of 85 for CAC, the frequency of healthy subjects with CAD-RADS less than two was significantly higher than the cases (P-value = 0.012), while the two groups were similar regarding CAD-RADS 3-5 (P-value = 0.83).
Conclusion: According to this study, the CAC score is a valuable means to detect CAD among CKD subjects. There is no significant difference in CAC between patients with substantial CAD-RADS in CKD and non-CKD patients. The cut-point of 85 for the CAC score was found valuable to diagnose CAD with over 80% sensitivity and specificity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


