Emily Barr, Justine Levesque, John Badir, Randall Dunston, Tamra Ranasinghe
{"title":"Unveiling the Uncommon: A Case Report of Horner's Syndrome as a Rare Glimpse Into Giant Cell Arteritis.","authors":"Emily Barr, Justine Levesque, John Badir, Randall Dunston, Tamra Ranasinghe","doi":"10.1155/crnm/2503963","DOIUrl":null,"url":null,"abstract":"<p><p>Giant cell arteritis (GCA) is an inflammatory vasculitis affecting large and medium-sized arteries, leading to complications such as arterial dissection, blindness, and stroke. Rarely, GCA presents with Horner's syndrome due to sympathetic neuron involvement from arterial inflammation. This case report discusses an 82-year-old female with hypertension, atrial fibrillation, and arthritis who presented with a 24 h history of right eye ptosis, blurred vision, dizziness, and aching eye pain. She had a mild headache and tenderness over the right temporomandibular joint but no temporal artery tenderness. Examination revealed right eye ptosis and miosis, indicative of Horner's syndrome, with no other neurological deficits. Lab results showed elevated ESR (68 mm/h) and CRP (16 mg/L). MRI with contrast revealed mild to moderate stenosis and enhancement in bilateral MCAs and basilar artery with inflammation in the right distal extracranial ICA, suggesting an inflammatory process. The patient was started on prednisone 40 mg daily. A temporal artery biopsy confirmed GCA with characteristic histopathological findings. Her prednisone dosage was increased to 60 mg/day, and she was started on tocilizumab. This case underscores the need to consider GCA in patients with Horner's syndrome and the importance of vessel wall imaging, as early corticosteroid treatment can prevent complications like vision loss and stroke.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2024 ","pages":"2503963"},"PeriodicalIF":0.9000,"publicationDate":"2024-12-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11651727/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crnm/2503963","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
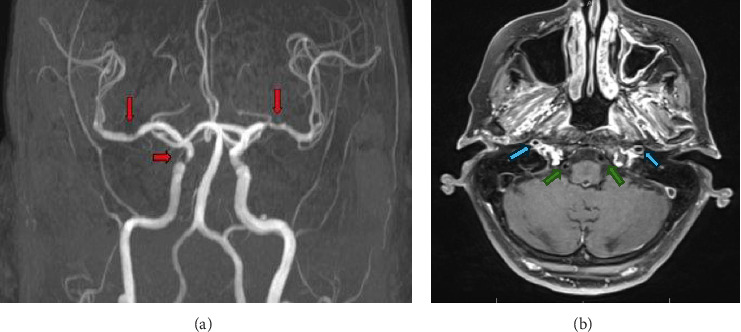
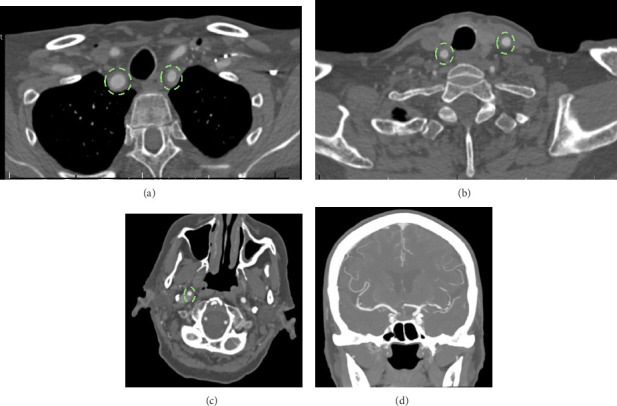
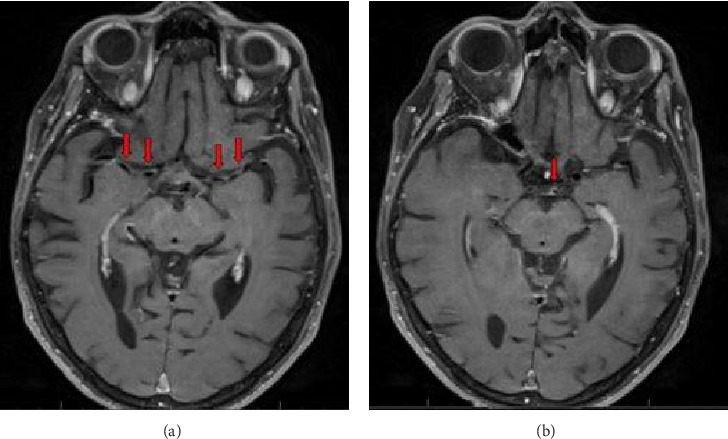
Giant cell arteritis (GCA) is an inflammatory vasculitis affecting large and medium-sized arteries, leading to complications such as arterial dissection, blindness, and stroke. Rarely, GCA presents with Horner's syndrome due to sympathetic neuron involvement from arterial inflammation. This case report discusses an 82-year-old female with hypertension, atrial fibrillation, and arthritis who presented with a 24 h history of right eye ptosis, blurred vision, dizziness, and aching eye pain. She had a mild headache and tenderness over the right temporomandibular joint but no temporal artery tenderness. Examination revealed right eye ptosis and miosis, indicative of Horner's syndrome, with no other neurological deficits. Lab results showed elevated ESR (68 mm/h) and CRP (16 mg/L). MRI with contrast revealed mild to moderate stenosis and enhancement in bilateral MCAs and basilar artery with inflammation in the right distal extracranial ICA, suggesting an inflammatory process. The patient was started on prednisone 40 mg daily. A temporal artery biopsy confirmed GCA with characteristic histopathological findings. Her prednisone dosage was increased to 60 mg/day, and she was started on tocilizumab. This case underscores the need to consider GCA in patients with Horner's syndrome and the importance of vessel wall imaging, as early corticosteroid treatment can prevent complications like vision loss and stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


