Two-transcript signature for differentiation and clinical outcomes in severe fever with thrombocytopenia syndrome (SFTS) patients: a double-blind, multicenter, validation study.
Nannan Xu, Sai Wen, Yongyuan Yao, Yanyan Guan, Lianhui Zhao, Lulu Yang, Hui Yang, Yishan He, Gang Wang
{"title":"Two-transcript signature for differentiation and clinical outcomes in severe fever with thrombocytopenia syndrome (SFTS) patients: a double-blind, multicenter, validation study.","authors":"Nannan Xu, Sai Wen, Yongyuan Yao, Yanyan Guan, Lianhui Zhao, Lulu Yang, Hui Yang, Yishan He, Gang Wang","doi":"10.1128/jcm.01282-24","DOIUrl":null,"url":null,"abstract":"<p><p>Severe fever with thrombocytopenia syndrome (SFTS) is an emerging infectious disease with a high mortality rate that is often underdiagnosed due to the limitations of current laboratory testing. Timely diagnosis and early identification of severe cases are crucial to improving patient outcomes and overall survival rates. This study aimed to evaluate the efficacy of two transcripts, IFI44L and PI3, in the early differentiation between SFTS virus (SFTSV) infection and bacterial sepsis, as well as in the prompt identification of severe cases during epidemic seasons. In a prospective study conducted between 1 May 2021 and 30 September 2022, we enrolled 225 patients who presented with acute fever and thrombocytopenia at four hospitals in Shandong Province, China. The two-transcript signature provided a clear distinction between SFTS and bacterial infection, achieving an area under the receiver operating characteristic curve of 0.961 (95% confidence interval [95% CI] 0.916-0.986), outperforming C-reactive protein (0.810 [95% CI 0.738-0.870]) and procalcitonin (0.764 [95% CI 0.687-0.830]). Importantly, the relative expression of the IFI44L gene was significantly elevated in fatal SFTS cases, with an area under the curve (AUC) of 0.820 (95% CI 0.727-0.914), indicating its potential as an early prognostic marker. Additionally, IFI44L and PI3 were identified as potential biomarkers for distinguishing SFTS patients with and without invasive pulmonary aspergillosis, with AUC values of 0.817 and 0.753, respectively. Our findings demonstrate that the two-transcript signature effectively distinguishes SFTSV infection from bacterial sepsis and helps identify high-risk individuals, guiding appropriate treatment during SFTS outbreak.</p>","PeriodicalId":15511,"journal":{"name":"Journal of Clinical Microbiology","volume":" ","pages":"e0128224"},"PeriodicalIF":5.4000,"publicationDate":"2025-01-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784442/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Microbiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1128/jcm.01282-24","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MICROBIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
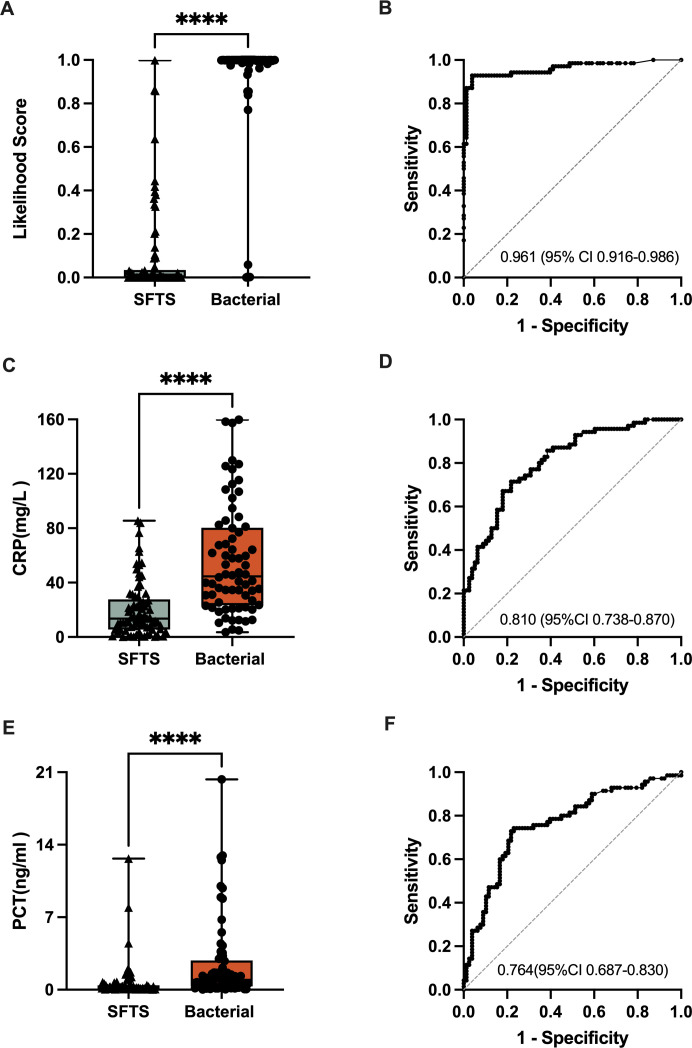
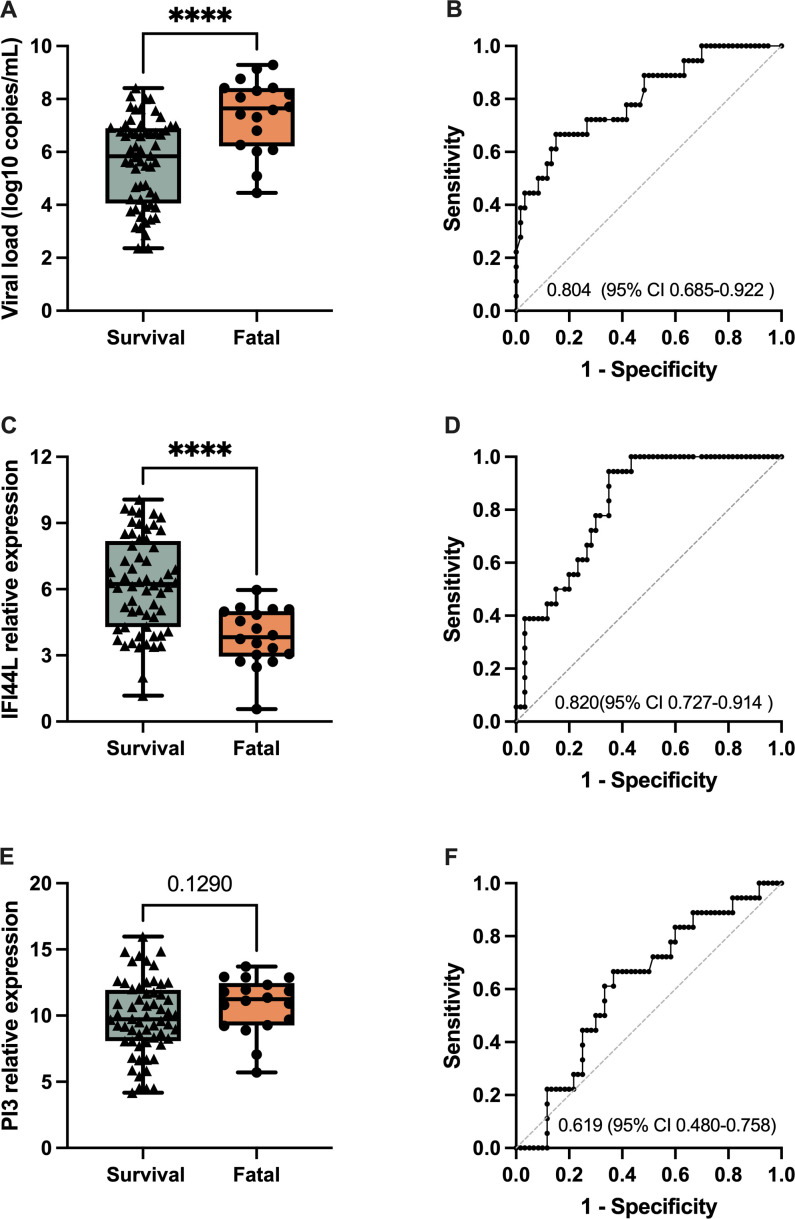
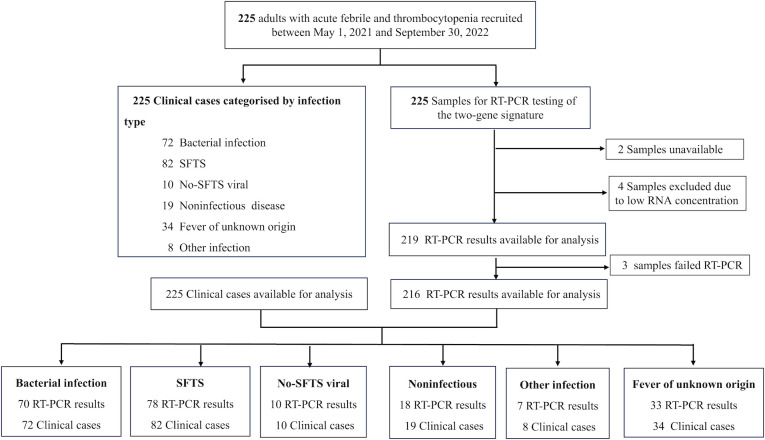
Severe fever with thrombocytopenia syndrome (SFTS) is an emerging infectious disease with a high mortality rate that is often underdiagnosed due to the limitations of current laboratory testing. Timely diagnosis and early identification of severe cases are crucial to improving patient outcomes and overall survival rates. This study aimed to evaluate the efficacy of two transcripts, IFI44L and PI3, in the early differentiation between SFTS virus (SFTSV) infection and bacterial sepsis, as well as in the prompt identification of severe cases during epidemic seasons. In a prospective study conducted between 1 May 2021 and 30 September 2022, we enrolled 225 patients who presented with acute fever and thrombocytopenia at four hospitals in Shandong Province, China. The two-transcript signature provided a clear distinction between SFTS and bacterial infection, achieving an area under the receiver operating characteristic curve of 0.961 (95% confidence interval [95% CI] 0.916-0.986), outperforming C-reactive protein (0.810 [95% CI 0.738-0.870]) and procalcitonin (0.764 [95% CI 0.687-0.830]). Importantly, the relative expression of the IFI44L gene was significantly elevated in fatal SFTS cases, with an area under the curve (AUC) of 0.820 (95% CI 0.727-0.914), indicating its potential as an early prognostic marker. Additionally, IFI44L and PI3 were identified as potential biomarkers for distinguishing SFTS patients with and without invasive pulmonary aspergillosis, with AUC values of 0.817 and 0.753, respectively. Our findings demonstrate that the two-transcript signature effectively distinguishes SFTSV infection from bacterial sepsis and helps identify high-risk individuals, guiding appropriate treatment during SFTS outbreak.
发热伴血小板减少综合征(SFTS)是一种死亡率高的新发传染病,由于目前实验室检测的局限性,往往未得到充分诊断。及时诊断和早期识别重症病例对于改善患者预后和总体生存率至关重要。本研究旨在评估两个转录本IFI44L和PI3在早期区分SFTS病毒(SFTSV)感染和细菌性脓毒症以及在流行季节及时识别重症病例方面的功效。在2021年5月1日至2022年9月30日期间进行的一项前瞻性研究中,我们在中国山东省的四家医院招募了225名出现急性发烧和血小板减少症的患者。双转录本签名提供了SFTS和细菌感染之间的明确区分,在接受者工作特征曲线下的面积为0.961(95%置信区间[95% CI] 0.916-0.986),优于c反应蛋白(0.810 [95% CI 0.738-0.870])和降钙素原(0.764 [95% CI 0.687-0.830])。重要的是,IFI44L基因的相对表达在致死性SFTS病例中显著升高,曲线下面积(AUC)为0.820 (95% CI 0.727-0.914),表明其可能作为早期预后标志物。此外,IFI44L和PI3被确定为区分有无侵袭性肺曲霉病的SFTS患者的潜在生物标志物,AUC值分别为0.817和0.753。我们的研究结果表明,双转录本签名可以有效区分SFTSV感染和细菌性败血症,并有助于识别高危个体,指导SFTS爆发期间的适当治疗。
期刊介绍:
The Journal of Clinical Microbiology® disseminates the latest research concerning the laboratory diagnosis of human and animal infections, along with the laboratory's role in epidemiology and the management of infectious diseases.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


