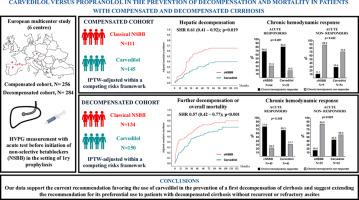
Carvedilol vs. propranolol for the prevention of decompensation and mortality in patients with compensated and decompensated cirrhosis
IF 26.8
1区 医学
Q1 GASTROENTEROLOGY & HEPATOLOGY
引用次数: 0
Abstract
Background and Aims
Data on the effectiveness of classical non-selective beta-blockers (cNSBB, i.e., propranolol and nadolol) versus carvedilol in patients with cirrhosis are scarce. The present study aimed to compare their potential for preventing decompensation and mortality in patients with compensated and decompensated cirrhosis.Methods
Multicenter retrospective study including compensated and decompensated cirrhotic patients with clinically significant portal hypertension, undergoing measurement of hepatic venous pressure gradient (HVPG) to assess acute hemodynamic response to intravenous propranolol (i.e., HVPG decrease≥10% from baseline value) prior to primary prophylaxis for variceal bleeding. Outcomes were adjusted using Inverse Probability of Treatment Weighting (IPTW) in a competitive risk framework.Results
A total of 540 patients with cirrhosis were included, 256 compensated (cNSBB n=111; carvedilol n=145) and 284 decompensated (cNSBB n=134; carvedilol n=150). Median follow-up was 36.3 (IQR 16.9-61.0) months and 30.7 (IQR 13.1-52.2) months, respectively. After covariate balancing with IPTW, carvedilol, compared to cNSBB, significantly reduced the risk of a first decompensation in compensated patients (SHR 0.61; 95% CI 0.41-0.92; p=0.019) and a combined endpoint of further decompensation/death in decompensated patients (SHR 0.57; 95% CI 0.42-0.77; p<0.0001). A second HVPG was conducted on 176 (68.8%, compensated) and 177 patients (62.3%, decompensated). Acute non-responders, both compensated (11.1% vs. 29.4%; p=0.422) and decompensated (16.0% vs. 43.6%: p=0.0247) patients, showed a higher likelihood of achieving a chronic hemodynamic response with carvedilol. The safety profile of each type of NSBB was comparable in both cohorts.Conclusions
Our data endorse the current recommendation favoring the use of carvedilol in the prevention of a first decompensation of cirrhosis and suggest extending the recommendation for its preferential use to patients with decompensated cirrhosis without recurrent or refractory ascites.IMPACT AND IMPLICATIONS
This study addresses a gap in the comparative effectiveness of classical non-selective beta-blockers (e.g., propranolol and nadolol) versus carvedilol in managing cirrhosis in both compensated and decompensated stages. Our results support the preferential use of carvedilol in both settings due to its superior efficacy in reducing first and further decompensation. However, the retrospective nature of the study and inherent selection biases advise caution against broadly applying these findings to patients with decompensated cirrhosis who exhibit signs of circulatory dysfunction or recurrent/refractory ascites.
背景和目的 有关经典非选择性β-受体阻滞剂(cNSBB,即普萘洛尔和纳多洛尔)与卡维地洛对肝硬化患者疗效的数据很少。本研究旨在比较这两种药物在预防代偿期和失代偿期肝硬化患者失代偿和死亡方面的潜力。方法:多中心回顾性研究包括代偿期和失代偿期肝硬化患者,这些患者均有临床症状明显的门静脉高压,在静脉曲张出血的一级预防治疗前均接受肝静脉压力梯度(HVPG)测量,以评估对静脉注射普萘洛尔的急性血流动力学反应(即 HVPG 从基线值下降≥10%)。结果共纳入540例肝硬化患者,其中256例为代偿期(cNSBB n=111;卡维地洛 n=145),284例为失代偿期(cNSBB n=134;卡维地洛 n=150)。中位随访时间分别为 36.3 个月(IQR 16.9-61.0)和 30.7 个月(IQR 13.1-52.2)。用 IPTW 平衡协变量后,与 cNSBB 相比,卡维地洛显著降低了代偿期患者首次失代偿的风险(SHR 0.61;95% CI 0.41-0.92;p=0.019)和失代偿期患者进一步失代偿/死亡的综合终点(SHR 0.57;95% CI 0.42-0.77;p<0.0001)。对 176 名患者(68.8%,代偿)和 177 名患者(62.3%,失代偿)进行了第二次 HVPG 分析。代偿期(11.1% vs. 29.4%;p=0.422)和失代偿期(16.0% vs. 43.6%:p=0.0247)急性无应答患者使用卡维地洛获得慢性血流动力学应答的可能性更高。结论我们的数据支持目前关于使用卡维地洛预防肝硬化首次失代偿的建议,并建议将优先使用卡维地洛的建议扩大到无复发性或难治性腹水的失代偿肝硬化患者、本研究弥补了传统非选择性β-受体阻滞剂(如普萘洛尔和纳多洛尔)与卡维地洛治疗代偿期和失代偿期肝硬化疗效比较的空白。我们的研究结果支持在这两种情况下优先使用卡维地洛,因为它在减少首次失代偿和进一步失代偿方面疗效更佳。然而,由于本研究具有回顾性和固有的选择偏差,我们建议不要将这些研究结果广泛应用于出现循环功能障碍或复发性/难治性腹水症状的失代偿期肝硬化患者。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊
Journal of Hepatology
医学-胃肠肝病学
CiteScore
46.10
自引率
4.30%
发文量
2325
审稿时长
30 days
期刊介绍:
The Journal of Hepatology is the official publication of the European Association for the Study of the Liver (EASL). It is dedicated to presenting clinical and basic research in the field of hepatology through original papers, reviews, case reports, and letters to the Editor. The Journal is published in English and may consider supplements that pass an editorial review.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


