{"title":"Triglycerides and the Risk of Atherosclerotic Cardiovascular Events Across Different Risk Categories.","authors":"Hiroyuki Mizuta, Masanobu Ishii, So Ikebe, Yasuhiro Otsuka, Yoshinori Yamanouchi, Taishi Nakamura, Kenichi Tsujita","doi":"10.5551/jat.65334","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>To investigate the association between triglyceride levels and major adverse cardiovascular events (MACE) in primary and secondary prevention cohorts.</p><p><strong>Methods: </strong>This retrospective study was conducted with a nationwide health insurance claims database, which included approximately 3.8 million participants with medical checkups between January 2005 and August 2020 in Japan. The participants were classified into primary prevention (n=3,415,522) and secondary prevention (n=29,806) cohorts based on cardiovascular or cerebrovascular disease history. Each participant was categorized as having very low (triglyceride <50 mg/dL), low normal (50-99), high normal (100-149), or hypertriglyceridemia (≥ 150). The primary prevention cohort was further stratified into low-, intermediate-, and high-risk groups according to atherosclerotic cardiovascular diseases risk. Outcome was MACE, including acute myocardial infarction (AMI), unstable angina, ischemic stroke, and cardiac death.</p><p><strong>Results: </strong>Over a mean follow-up of 3.25 years, 0.3% and 2.6% MACE occurred in primary and secondary prevention, respectively. Hypertriglyceridemia was associated with high risk of MACE in the primary prevention, but not in the secondary prevention. A significant interaction was observed between prevention categories and the association of TG levels with MACE in those with TG <150 mg/dL and ischemic stroke in those with TG ≥ 150 mg/dL. The population-attributable fraction for hypertriglyceridemia in primary prevention was 4.1% for MACE. In primary prevention, lower risks of AMI were observed in the lower TG category compared to the current threshold.</p><p><strong>Conclusions: </strong>This study suggests distinct triglyceride thresholds for MACE risk in primary and secondary prevention cohorts, requiring further prospective validation for clinical implementation.</p>","PeriodicalId":15128,"journal":{"name":"Journal of atherosclerosis and thrombosis","volume":" ","pages":"786-803"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237766/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of atherosclerosis and thrombosis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5551/jat.65334","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: To investigate the association between triglyceride levels and major adverse cardiovascular events (MACE) in primary and secondary prevention cohorts.
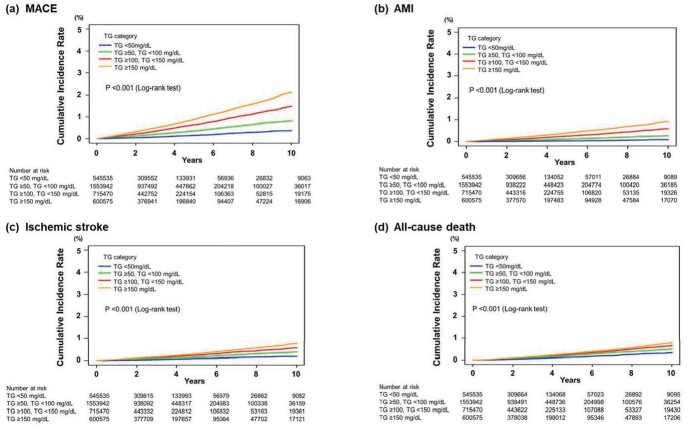
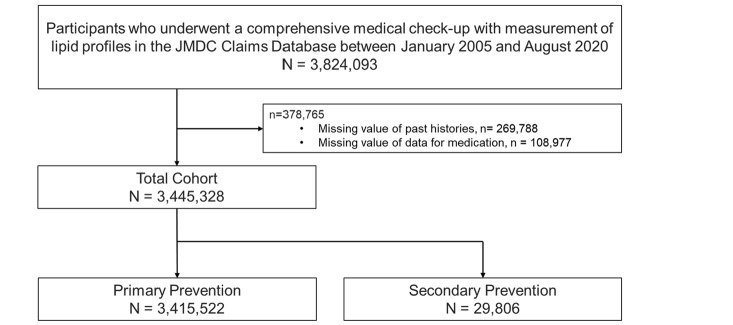
Methods: This retrospective study was conducted with a nationwide health insurance claims database, which included approximately 3.8 million participants with medical checkups between January 2005 and August 2020 in Japan. The participants were classified into primary prevention (n=3,415,522) and secondary prevention (n=29,806) cohorts based on cardiovascular or cerebrovascular disease history. Each participant was categorized as having very low (triglyceride <50 mg/dL), low normal (50-99), high normal (100-149), or hypertriglyceridemia (≥ 150). The primary prevention cohort was further stratified into low-, intermediate-, and high-risk groups according to atherosclerotic cardiovascular diseases risk. Outcome was MACE, including acute myocardial infarction (AMI), unstable angina, ischemic stroke, and cardiac death.
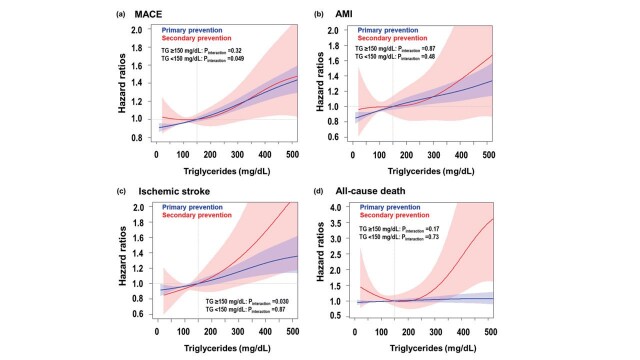
Results: Over a mean follow-up of 3.25 years, 0.3% and 2.6% MACE occurred in primary and secondary prevention, respectively. Hypertriglyceridemia was associated with high risk of MACE in the primary prevention, but not in the secondary prevention. A significant interaction was observed between prevention categories and the association of TG levels with MACE in those with TG <150 mg/dL and ischemic stroke in those with TG ≥ 150 mg/dL. The population-attributable fraction for hypertriglyceridemia in primary prevention was 4.1% for MACE. In primary prevention, lower risks of AMI were observed in the lower TG category compared to the current threshold.
Conclusions: This study suggests distinct triglyceride thresholds for MACE risk in primary and secondary prevention cohorts, requiring further prospective validation for clinical implementation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


