Roberta Zupo, Beatrice Poggi, Nicole Caggiano, Giulio Varrone, Fabio Castellana, Silvia Natoli, Rodolfo Sardone, Antonio Nardone, Chiara Pavese
{"title":"Methods of diagnosis and rehabilitation of dysphagia in patients with spinal cord injury: a systematic review.","authors":"Roberta Zupo, Beatrice Poggi, Nicole Caggiano, Giulio Varrone, Fabio Castellana, Silvia Natoli, Rodolfo Sardone, Antonio Nardone, Chiara Pavese","doi":"10.23736/S1973-9087.24.08614-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Latest epidemiological metrics put a global prevalence of 20.6 million people suffering from spinal cord injury (SCI), leading to a burden of functional disability, deterioration in quality of life and reduced life expectancy. A thorough statement of diagnostic methods and treatment protocols for swallowing disorders after SCI stands as a major priority to streamline patient care and cost-sharing. Here we have provided a systematic overview of the evidence on diagnostic and rehabilitation protocols of dysphagia in the SCI population.</p><p><strong>Evidence acquisition: </strong>The literature was searched in six electronic databases up to April 30<sup>th</sup>, 2024. Screening the 521 retrieved articles for inclusion criteria resulted in the selection of 43 studies that reported assessment tools and rehabilitation protocols for dysphagia in patients with SCI. Two researchers extracted the data in parallel, and inter-rater reliability (IRR) was used to estimate inter-coder agreement and then κ statistic to measure accuracy and precision. Based on PRISMA concepts and quality assessment steps, a k coefficient of at least 0.9 was obtained in all data extraction steps. All reports were assessed for risk of bias using the NIH Quality Assessment Toolkit. The study protocol was registered on PROSPERO (CRD42023449137).</p><p><strong>Evidence synthesis: </strong>Dysphagia assessment methods were collected and grouped into four different macro categories (clinical assessment, rating scale, self-reported questionnaire, and instrumental assessment). It was found that the Bedside Swallow Evaluation (BSE) for the clinical assessment category (50%), the Bazaz score (32.5%) for the rating scale category, the Eating Assessment Tool-10 (EAT-10) (44.4%) for the self-reported questionnaire category, and the Videofluoroscopic Study of Swallowing (VFSS) (48.9%) for the instrumental assessment category were the most representative tools. The rehabilitation protocols described included either an early oral feeding exclusion or a consistency-modified oral intake, postural adaptations, oxygen therapy with a high-flow nasal cannula combined with indirect/direct therapy, specific exercises, and neuromuscular electrical stimulation.</p><p><strong>Conclusions: </strong>Methods of diagnosis and rehabilitation protocols for dysphagia in SCI patients appear inconsistent. Further rigorous studies are needed to achieve better clinical handling in SCI settings while lowering the load of patient morbidity and related healthcare costs.</p>","PeriodicalId":12044,"journal":{"name":"European journal of physical and rehabilitation medicine","volume":" ","pages":"41-51"},"PeriodicalIF":3.4000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11919461/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of physical and rehabilitation medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.23736/S1973-9087.24.08614-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Latest epidemiological metrics put a global prevalence of 20.6 million people suffering from spinal cord injury (SCI), leading to a burden of functional disability, deterioration in quality of life and reduced life expectancy. A thorough statement of diagnostic methods and treatment protocols for swallowing disorders after SCI stands as a major priority to streamline patient care and cost-sharing. Here we have provided a systematic overview of the evidence on diagnostic and rehabilitation protocols of dysphagia in the SCI population.
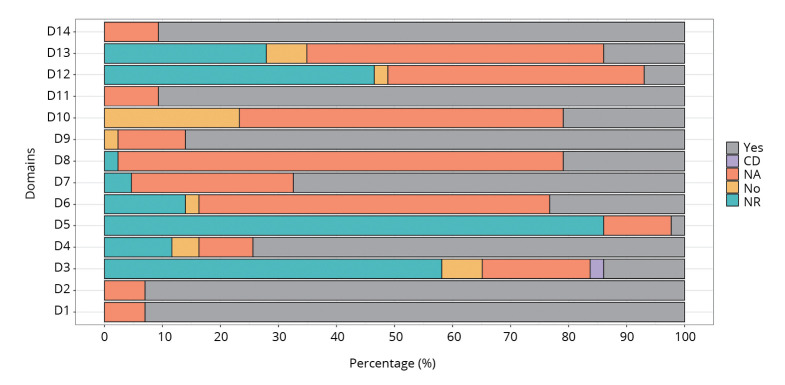
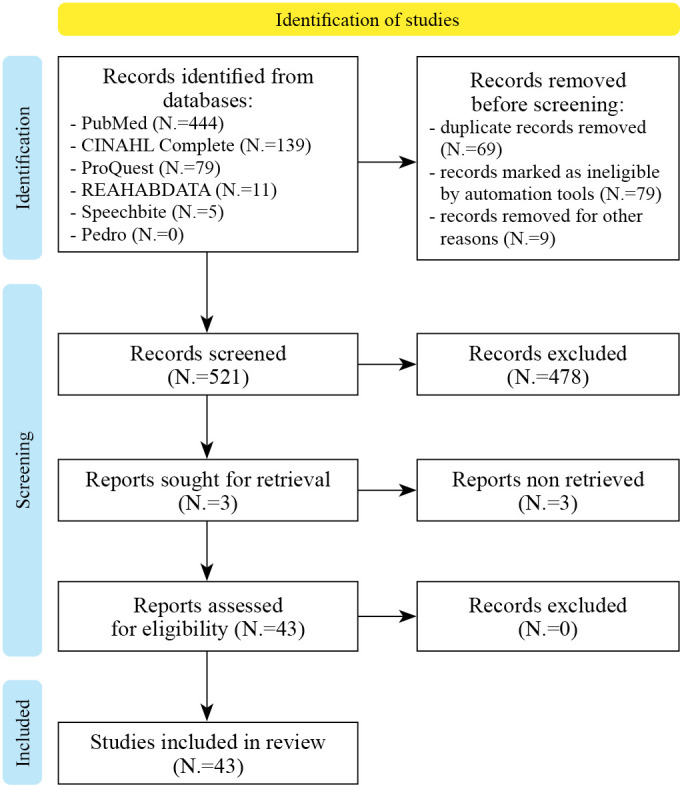
Evidence acquisition: The literature was searched in six electronic databases up to April 30th, 2024. Screening the 521 retrieved articles for inclusion criteria resulted in the selection of 43 studies that reported assessment tools and rehabilitation protocols for dysphagia in patients with SCI. Two researchers extracted the data in parallel, and inter-rater reliability (IRR) was used to estimate inter-coder agreement and then κ statistic to measure accuracy and precision. Based on PRISMA concepts and quality assessment steps, a k coefficient of at least 0.9 was obtained in all data extraction steps. All reports were assessed for risk of bias using the NIH Quality Assessment Toolkit. The study protocol was registered on PROSPERO (CRD42023449137).
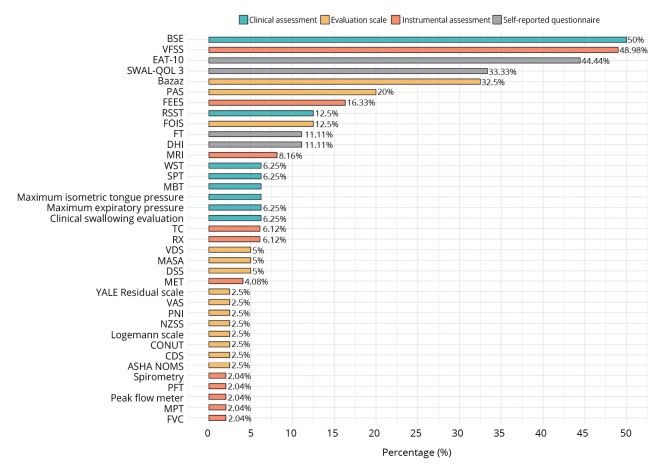
Evidence synthesis: Dysphagia assessment methods were collected and grouped into four different macro categories (clinical assessment, rating scale, self-reported questionnaire, and instrumental assessment). It was found that the Bedside Swallow Evaluation (BSE) for the clinical assessment category (50%), the Bazaz score (32.5%) for the rating scale category, the Eating Assessment Tool-10 (EAT-10) (44.4%) for the self-reported questionnaire category, and the Videofluoroscopic Study of Swallowing (VFSS) (48.9%) for the instrumental assessment category were the most representative tools. The rehabilitation protocols described included either an early oral feeding exclusion or a consistency-modified oral intake, postural adaptations, oxygen therapy with a high-flow nasal cannula combined with indirect/direct therapy, specific exercises, and neuromuscular electrical stimulation.
Conclusions: Methods of diagnosis and rehabilitation protocols for dysphagia in SCI patients appear inconsistent. Further rigorous studies are needed to achieve better clinical handling in SCI settings while lowering the load of patient morbidity and related healthcare costs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


