Nayla Léveillé, Floriane Point, Josée Houde, Michael Hall, Hafid Souhaline, Marie-Andrée Leblanc, Pierre-Marie Akochy, Simon Grandjean Lapierre
{"title":"<i>Mycobacterium tuberculosis</i> pseudo-outbreak due to laboratory cross-contamination: A molecular epidemiology outbreak investigation.","authors":"Nayla Léveillé, Floriane Point, Josée Houde, Michael Hall, Hafid Souhaline, Marie-Andrée Leblanc, Pierre-Marie Akochy, Simon Grandjean Lapierre","doi":"10.14745/ccdr.v50i12da03","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mycobacterial culture is routinely performed to diagnose tuberculosis (TB) in Canada. Globally, meta-analyses suggest that up to 2% of positive cultures are falsely positive for <i>Mycobacterium tuberculosis</i> due to laboratory cross-contamination. Five patients from distinct clinical institutions in Montréal were diagnosed with culture-positive TB as their clinical samples were processed in a centralized mycobacteria laboratory. Cross-contamination was suspected due to culture positivity in an organ donor with low TB pre-test probability. We describe a TB pseudo-outbreak due to laboratory cross-contamination and assess the role of conventional typing (i.e., mycobacterial interspersed repetitive unit variable number of tandem repeats [MIRU-VNTR]) and whole-genome sequencing (WGS) in supporting the investigation.</p><p><strong>Methods: </strong>Patients' epidemiological risk factors and clinical presentations were reviewed. The trajectories of pre- and per-analytic samples were retraced to identify potential cross-contamination events. Tuberculosis isolates were characterized by MIRU-VNTR and WGS using Oxford Nanopore Technology (ONT). The bioinformatic pipeline tbpore (v0.7.1) cluster was used for phylogenetic analyses.</p><p><strong>Results: </strong>Two patients had previous exposure to endemic settings and clinical symptoms compatible with TB. Culture media inoculation overlapped in time for four patients, including one with suspected pulmonary cavitary disease and an organ donor whose organs had been transplanted in three different receivers. The MIRU-VNTR and WGS typing confirmed isolates from those four patients to be identical.</p><p><strong>Conclusion: </strong>Clinical, laboratory and molecular typing data, including results from ONT sequencing, were considered sufficiently robust to confirm laboratory cross-contamination and TB therapy was discontinued including in all organ transplant recipients.</p>","PeriodicalId":94304,"journal":{"name":"Canada communicable disease report = Releve des maladies transmissibles au Canada","volume":"50 12","pages":"430-435"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11629878/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canada communicable disease report = Releve des maladies transmissibles au Canada","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14745/ccdr.v50i12da03","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Mycobacterial culture is routinely performed to diagnose tuberculosis (TB) in Canada. Globally, meta-analyses suggest that up to 2% of positive cultures are falsely positive for Mycobacterium tuberculosis due to laboratory cross-contamination. Five patients from distinct clinical institutions in Montréal were diagnosed with culture-positive TB as their clinical samples were processed in a centralized mycobacteria laboratory. Cross-contamination was suspected due to culture positivity in an organ donor with low TB pre-test probability. We describe a TB pseudo-outbreak due to laboratory cross-contamination and assess the role of conventional typing (i.e., mycobacterial interspersed repetitive unit variable number of tandem repeats [MIRU-VNTR]) and whole-genome sequencing (WGS) in supporting the investigation.
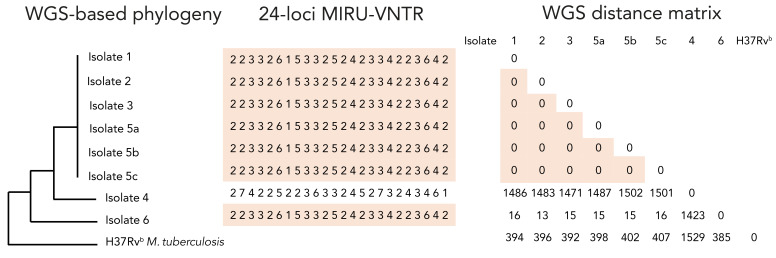
Methods: Patients' epidemiological risk factors and clinical presentations were reviewed. The trajectories of pre- and per-analytic samples were retraced to identify potential cross-contamination events. Tuberculosis isolates were characterized by MIRU-VNTR and WGS using Oxford Nanopore Technology (ONT). The bioinformatic pipeline tbpore (v0.7.1) cluster was used for phylogenetic analyses.
Results: Two patients had previous exposure to endemic settings and clinical symptoms compatible with TB. Culture media inoculation overlapped in time for four patients, including one with suspected pulmonary cavitary disease and an organ donor whose organs had been transplanted in three different receivers. The MIRU-VNTR and WGS typing confirmed isolates from those four patients to be identical.
Conclusion: Clinical, laboratory and molecular typing data, including results from ONT sequencing, were considered sufficiently robust to confirm laboratory cross-contamination and TB therapy was discontinued including in all organ transplant recipients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


