Amlodipine in the HRT cycle for frozen embryo transfer to correct uterine artery resistance in women with prior implantation failure: a randomized controlled trial.
{"title":"Amlodipine in the HRT cycle for frozen embryo transfer to correct uterine artery resistance in women with prior implantation failure: a randomized controlled trial.","authors":"Nazli Navali, Elham Eghbali, Laya Farzadi, Aliyeh Ghasemzadeh, Kobra Hamdi, Parvin Hakimi, Hojat Ghasemnejad-Berenji, Sonia Sadeghpour","doi":"10.5653/cerm.2024.07129","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>For successful embryo implantation in women with high pulsatility, uterine vascular resistance and pulsatility must be reduced. We examined the effects of amlodipine on uterine pulsatility index (PI), resistance index (RI), and embryo transfer (ET) outcomes in women with prior implantation failure and at least one elevated uterine PI measurement (especially higher than 3).</p><p><strong>Methods: </strong>Between February and November 2023, our reproductive facility conducted a single-center randomized clinical trial, enrolling 100 patients with previous implantation failure and at least one uterine PI measurement exceeding 3. Participants were randomly assigned to receive either amlodipine (5 mg) or placebo (n=50 per group). Hormone replacement therapy was the predominant method for endometrial preparation. Transvaginal ultrasonography was used to measure uterine artery resistance and pulsatility on day 1 or 2 of menstruation. Women in the amlodipine group received 5 mg nightly. Following repeat transvaginal ultrasound to assess PI and RI, ET was performed. If a positive pregnancy test was obtained, treatment continued for a total of 7 weeks.</p><p><strong>Results: </strong>Amlodipine reduced blood flow indices in the uterine artery. Among placebo recipients, 18% tested positive for beta-human chorionic gonadotropin, compared to 26% of medication recipients. However, this difference was statistically insignificant (p=0.472). Gestational sacs were observed in 12% of the placebo group and 22% of the medication group, but this difference was also insignificant (p=0.28).</p><p><strong>Conclusion: </strong>Amlodipine appears to reduce uterine pulsatility and resistance during ET. Despite the absence of significant differences in pregnancy outcomes, this promising drug merits further study in women with implantation failure.</p>","PeriodicalId":46409,"journal":{"name":"Clinical and Experimental Reproductive Medicine-CERM","volume":" ","pages":"141-149"},"PeriodicalIF":1.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12149864/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Reproductive Medicine-CERM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5653/cerm.2024.07129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: For successful embryo implantation in women with high pulsatility, uterine vascular resistance and pulsatility must be reduced. We examined the effects of amlodipine on uterine pulsatility index (PI), resistance index (RI), and embryo transfer (ET) outcomes in women with prior implantation failure and at least one elevated uterine PI measurement (especially higher than 3).
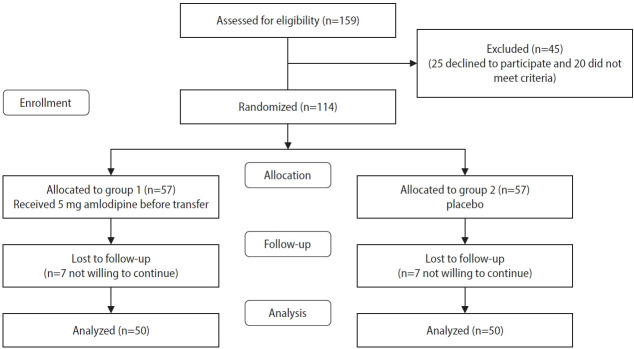
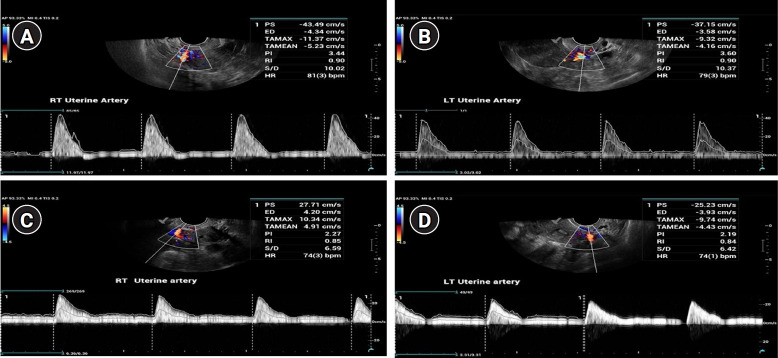
Methods: Between February and November 2023, our reproductive facility conducted a single-center randomized clinical trial, enrolling 100 patients with previous implantation failure and at least one uterine PI measurement exceeding 3. Participants were randomly assigned to receive either amlodipine (5 mg) or placebo (n=50 per group). Hormone replacement therapy was the predominant method for endometrial preparation. Transvaginal ultrasonography was used to measure uterine artery resistance and pulsatility on day 1 or 2 of menstruation. Women in the amlodipine group received 5 mg nightly. Following repeat transvaginal ultrasound to assess PI and RI, ET was performed. If a positive pregnancy test was obtained, treatment continued for a total of 7 weeks.
Results: Amlodipine reduced blood flow indices in the uterine artery. Among placebo recipients, 18% tested positive for beta-human chorionic gonadotropin, compared to 26% of medication recipients. However, this difference was statistically insignificant (p=0.472). Gestational sacs were observed in 12% of the placebo group and 22% of the medication group, but this difference was also insignificant (p=0.28).
Conclusion: Amlodipine appears to reduce uterine pulsatility and resistance during ET. Despite the absence of significant differences in pregnancy outcomes, this promising drug merits further study in women with implantation failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


