Kathiresan Jeyashree, Jeromie W V Thangaraj, Devika Shanmugasundaram, Sri Lakshmi Priya Giridharan, Sumit Pandey, Prema Shanmugasundaram, Sabarinathan Ramasamy, Venkateshprabhu Janagaraj, Sivavallinathan Arunachalam, Rahul Sharma, Vaibhav Shah, Bhavani Shankara Bagepally, Joshua Chadwick, Hemant Deepak Shewade, Aniket Chowdhury, Swati Iyer, Raghuram Rao, Sanjay K Mattoo, Manoj V Murhekar
{"title":"Cost of TB care and equity in distribution of catastrophic TB care costs across income quintiles in India.","authors":"Kathiresan Jeyashree, Jeromie W V Thangaraj, Devika Shanmugasundaram, Sri Lakshmi Priya Giridharan, Sumit Pandey, Prema Shanmugasundaram, Sabarinathan Ramasamy, Venkateshprabhu Janagaraj, Sivavallinathan Arunachalam, Rahul Sharma, Vaibhav Shah, Bhavani Shankara Bagepally, Joshua Chadwick, Hemant Deepak Shewade, Aniket Chowdhury, Swati Iyer, Raghuram Rao, Sanjay K Mattoo, Manoj V Murhekar","doi":"10.1186/s41256-024-00392-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tuberculosis (TB) poses a significant social and economic burden to households of persons with TB (PwTB). Despite free diagnosis and care under the National TB Elimination Programme (NTEP), individuals often experience significant out-of-pocket expenditure and lost productivity, causing financial catastrophe. We estimated the costs incurred by the PwTB during TB care and identified the factors associated with the costs.</p><p><strong>Methods: </strong>In our cross-sectional study, we used multi-stage sampling to select PwTB notified under the NTEP, whose treatment outcome was declared between May 2022 and February 2023. Total patient costs were measured through direct medical, non-medical and indirect costs. Catastrophic costs were defined as expenditure on TB care > 20% of the annual household income. We determined the factors influencing the total cost of TB care using median regression. We plotted concentration curves to depict the equity in distribution of catastrophic costs across income quintiles. We used a cluster-adjusted, generalized model to determine the factors associated with catastrophic costs.</p><p><strong>Results: </strong>The mean (SD) age of the 1407 PwTB interviewed was 40.8 (16.8) years. Among them, 865 (61.5%) were male, and 786 (55.9%) were economically active. Thirty-four (2.4%) had Drug Resistant TB (DRTB), and 258 (18.3%) had been hospitalized for TB. The median (Interquartile range [IQR] and 95% confidence interval [CI]) of total costs of TB care was US$386.1 (130.8, 876.9). Direct costs accounted for 34% of the total costs, with a median of US$78.4 (43.3, 153.6), while indirect costs had a median of US$279.8 (18.9,699.4). PwTB < 60 years of age (US$446.1; 370.4, 521.8), without health insurance (US$464.2; 386.7, 541.6), and those hospitalized(US$900.4; 700.2, 1100.6) for TB experienced higher median costs. Catastrophic costs, experienced by 45% of PwTB, followed a pro-poor distribution. Hospitalized PwTB (adjusted prevalence ratio [aPR] = 1.9; 1.6, 2.2) and those notified from the private sector (aPR = 1.4; 1.1, 1.8) were more likely to incur catastrophic costs.</p><p><strong>Conclusions: </strong>PwTB in India incur high costs mainly due to lost productivity and hospitalization. Nearly half of them experience catastrophic costs, especially those from poorer economic quintiles. Enabling early notification of TB, expanding the coverage of health insurance schemes to include PwTB, and implementing TB sensitive strategies to address social determinants of TB may significantly reduce catastrophic costs incurred by PwTB.</p>","PeriodicalId":52405,"journal":{"name":"Global Health Research and Policy","volume":"9 1","pages":"51"},"PeriodicalIF":4.6000,"publicationDate":"2024-12-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11626761/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health Research and Policy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41256-024-00392-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Tuberculosis (TB) poses a significant social and economic burden to households of persons with TB (PwTB). Despite free diagnosis and care under the National TB Elimination Programme (NTEP), individuals often experience significant out-of-pocket expenditure and lost productivity, causing financial catastrophe. We estimated the costs incurred by the PwTB during TB care and identified the factors associated with the costs.
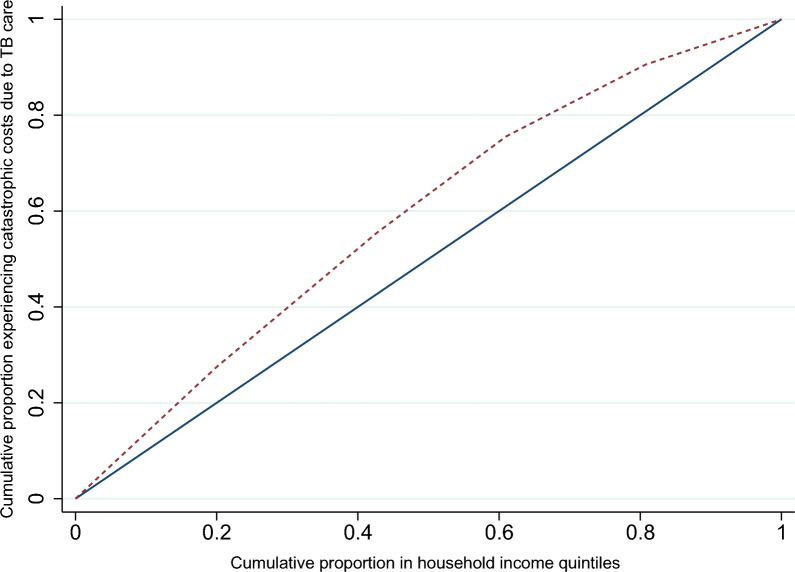
Methods: In our cross-sectional study, we used multi-stage sampling to select PwTB notified under the NTEP, whose treatment outcome was declared between May 2022 and February 2023. Total patient costs were measured through direct medical, non-medical and indirect costs. Catastrophic costs were defined as expenditure on TB care > 20% of the annual household income. We determined the factors influencing the total cost of TB care using median regression. We plotted concentration curves to depict the equity in distribution of catastrophic costs across income quintiles. We used a cluster-adjusted, generalized model to determine the factors associated with catastrophic costs.
Results: The mean (SD) age of the 1407 PwTB interviewed was 40.8 (16.8) years. Among them, 865 (61.5%) were male, and 786 (55.9%) were economically active. Thirty-four (2.4%) had Drug Resistant TB (DRTB), and 258 (18.3%) had been hospitalized for TB. The median (Interquartile range [IQR] and 95% confidence interval [CI]) of total costs of TB care was US$386.1 (130.8, 876.9). Direct costs accounted for 34% of the total costs, with a median of US$78.4 (43.3, 153.6), while indirect costs had a median of US$279.8 (18.9,699.4). PwTB < 60 years of age (US$446.1; 370.4, 521.8), without health insurance (US$464.2; 386.7, 541.6), and those hospitalized(US$900.4; 700.2, 1100.6) for TB experienced higher median costs. Catastrophic costs, experienced by 45% of PwTB, followed a pro-poor distribution. Hospitalized PwTB (adjusted prevalence ratio [aPR] = 1.9; 1.6, 2.2) and those notified from the private sector (aPR = 1.4; 1.1, 1.8) were more likely to incur catastrophic costs.
Conclusions: PwTB in India incur high costs mainly due to lost productivity and hospitalization. Nearly half of them experience catastrophic costs, especially those from poorer economic quintiles. Enabling early notification of TB, expanding the coverage of health insurance schemes to include PwTB, and implementing TB sensitive strategies to address social determinants of TB may significantly reduce catastrophic costs incurred by PwTB.
期刊介绍:
Global Health Research and Policy, an open-access, multidisciplinary journal, publishes research on various aspects of global health, addressing topics like health equity, health systems and policy, social determinants of health, disease burden, population health, and other urgent global health issues. It serves as a forum for high-quality research focused on regional and global health improvement, emphasizing solutions for health equity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


