{"title":"Video-Oculography for Enhancing the Diagnostic Accuracy of Early Oculomotor Dysfunction in Progressive Supranuclear Palsy.","authors":"Harshad Chovatiya, Kanchana Pillai, Chakradhar Reddy, Amiya Thalakkattu, Ayana Avarachan, Manas Chacko, Asha Kishore","doi":"10.14802/jmd.24171","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Oculomotor impairment is an important diagnostic feature of progressive supranuclear palsy (PSP) and PSP subtypes. We assessed the role of video-oculography (VOG) in confirming clinically suspected slow saccades in PSP and differentiating PSP from Parkinson's disease (PD). We also measured the correlation of both saccadic velocity and latency in PSP patients with scores on the PSP Rating Scale, Montreal Cognitive Assessment, and frontal assessment battery. We assessed the frequency of apraxia of eyelid opening (ALO) and reflex blepharospasm in PSP and PD patients.</p><p><strong>Methods: </strong>A total of 112 PSP patients with slow saccades but not gaze palsy, 50 PD patients, and 50 healthy controls (HCs) were recruited. The Movement Disorders Society task force-PSP and PD criteria were used for the diagnoses. All the subjects underwent VOG.</p><p><strong>Results: </strong>Horizontal and vertical saccadic velocities and latencies differentiated PSP patients from PD patients and HCs (p<0.001). Vertical saccadic velocity and latency accurately differentiated PSP with predominant parkinsonism (PSP-P) patients from PD patients (p<0.001 and 0.012, respectively). A couple of vertical and horizontal saccadic velocities differentiated PSP-Richardson's syndrome (PSP-RS) patients from PSP-P patients (vertical velocity of left eye: p=0.024; horizontal velocity of right eye: p=0.030). In vertical gaze, the mean velocity cutoff showed good sensitivity and specificity in differentiating PSP patients from HCs and PD patients. Prolonged horizontal gaze latency was associated with more severe PSP and worse global cognitive and frontal dysfunction. ALO and reflex blepharospasm were observed only in PSP patients.</p><p><strong>Conclusion: </strong>VOG is useful for confirming slow saccades in PSP-RS and PSP-P patients and for differentiating PSP-P patients from PD patients. Prolonged horizontal gaze latency was associated with more severe PSP and worse cognitive dysfunction. ALO and reflex blepharospasm were observed only in PSP patients.</p>","PeriodicalId":16372,"journal":{"name":"Journal of Movement Disorders","volume":" ","pages":"77-86"},"PeriodicalIF":2.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11824506/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Movement Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14802/jmd.24171","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/9 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Oculomotor impairment is an important diagnostic feature of progressive supranuclear palsy (PSP) and PSP subtypes. We assessed the role of video-oculography (VOG) in confirming clinically suspected slow saccades in PSP and differentiating PSP from Parkinson's disease (PD). We also measured the correlation of both saccadic velocity and latency in PSP patients with scores on the PSP Rating Scale, Montreal Cognitive Assessment, and frontal assessment battery. We assessed the frequency of apraxia of eyelid opening (ALO) and reflex blepharospasm in PSP and PD patients.
Methods: A total of 112 PSP patients with slow saccades but not gaze palsy, 50 PD patients, and 50 healthy controls (HCs) were recruited. The Movement Disorders Society task force-PSP and PD criteria were used for the diagnoses. All the subjects underwent VOG.
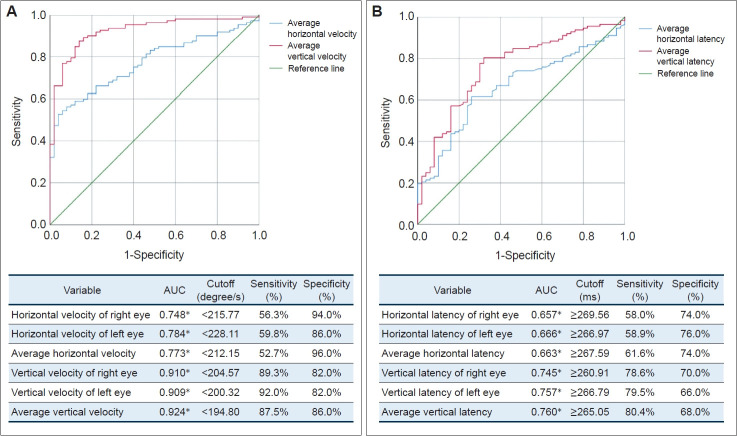
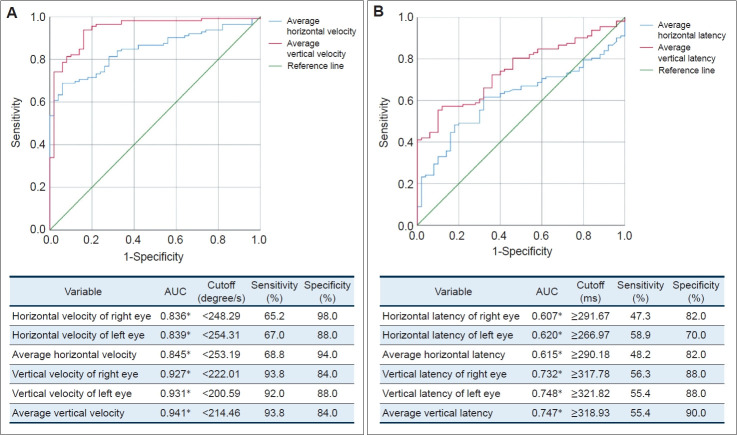
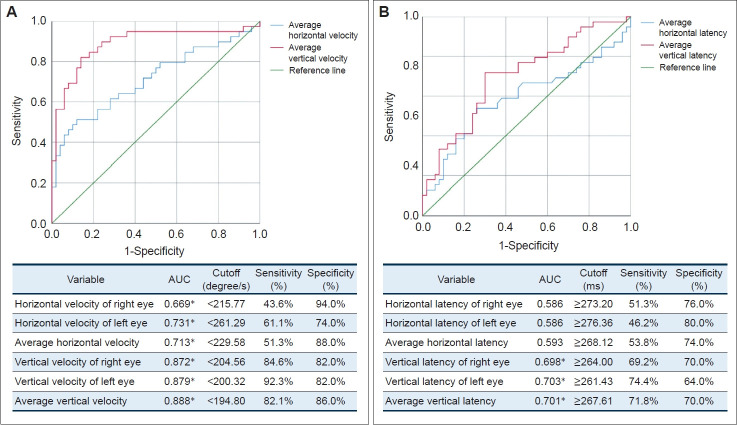
Results: Horizontal and vertical saccadic velocities and latencies differentiated PSP patients from PD patients and HCs (p<0.001). Vertical saccadic velocity and latency accurately differentiated PSP with predominant parkinsonism (PSP-P) patients from PD patients (p<0.001 and 0.012, respectively). A couple of vertical and horizontal saccadic velocities differentiated PSP-Richardson's syndrome (PSP-RS) patients from PSP-P patients (vertical velocity of left eye: p=0.024; horizontal velocity of right eye: p=0.030). In vertical gaze, the mean velocity cutoff showed good sensitivity and specificity in differentiating PSP patients from HCs and PD patients. Prolonged horizontal gaze latency was associated with more severe PSP and worse global cognitive and frontal dysfunction. ALO and reflex blepharospasm were observed only in PSP patients.
Conclusion: VOG is useful for confirming slow saccades in PSP-RS and PSP-P patients and for differentiating PSP-P patients from PD patients. Prolonged horizontal gaze latency was associated with more severe PSP and worse cognitive dysfunction. ALO and reflex blepharospasm were observed only in PSP patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


