Comparative Analysis of Stent-Assisted Versus Non-Stent-Assisted Coiling in the Management of Ruptured Intracranial Aneurysms: A Systematic Review and Meta-Analysis.
{"title":"Comparative Analysis of Stent-Assisted Versus Non-Stent-Assisted Coiling in the Management of Ruptured Intracranial Aneurysms: A Systematic Review and Meta-Analysis.","authors":"Yu-Hu Ma, Yong-Lin He, Xiao-Yue Zhang, Rui Shang, Hai-Tao Hu, Ting Wang, Sen Lin, Ya-Wen Pan, Chang-Wei Zhang","doi":"10.1007/s12975-024-01314-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To systematically evaluate the safety and efficacy of SAC compared to non-SAC in the treatment of RIA, integrating evidence from high-quality studies to guide clinical practice.</p><p><strong>Methods: </strong>A meta-analysis was conducted to compare SAC with coiling alone and BAC in the treatment of RIA. Primary outcomes were immediate and follow-up aneurysm occlusion rates, along with perioperative hemorrhagic and ischemic complication rates.</p><p><strong>Results: </strong>A total of thirteen retrospective cohort studies were included, comprising 3,086 patients, with 1,078 in the SAC group and 2,008 in the non-SAC group. The immediate complete occlusion rates were similar between the SAC and non-SAC groups (59.1% vs. 61.4%; RR = 1.00; 95% CI [0.94, 1.07]; p = 0.92). However, the SAC group demonstrated a significantly higher long-term complete occlusion rate (61.3% vs. 40.6%; RR = 1.44; 95% CI [1.22, 1.69]; p < 0.001). The incidence of ischemic complications was greater in the SAC group (12.2% vs. 10.0%; RR = 1.68; 95% CI [1.37, 2.07]; p < 0.001), as was the incidence of hemorrhagic complications (7.3% vs. 5.1%; RR = 1.55; 95% CI [1.15, 2.08]; p = 0.004). Perioperative mortality was also elevated in the SAC group (6.7% vs. 6.8%; RR = 1.37; 95% CI [1.00, 1.88]; p = 0.048), with a non-significant trend towards higher long-term mortality (9.8% vs. 9.2%; RR = 1.35; 95% CI [0.98, 1.87]; p = 0.068). Functional outcomes at discharge (76.0% vs. 71.0%; RR = 0.97; 95% CI [0.92, 1.02]; p = 0.237), six months (57.8% vs. 60.8%; RR = 0.93; 95% CI [0.81, 1.07]; p = 0.296), and at the last follow-up (RR = 1.01; 95% CI [0.97, 1.06]; p = 0.592) were comparable between the two groups.</p><p><strong>Conclusions: </strong>SAC significantly improves long-term occlusion rates for RIA compared to non-SAC, despite a higher incidence of complications. Careful patient selection and optimization of antiplatelet therapy may enhance the safety and efficacy of SAC for RIA treatment.</p>","PeriodicalId":23237,"journal":{"name":"Translational Stroke Research","volume":" ","pages":"1424-1439"},"PeriodicalIF":4.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202655/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational Stroke Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12975-024-01314-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To systematically evaluate the safety and efficacy of SAC compared to non-SAC in the treatment of RIA, integrating evidence from high-quality studies to guide clinical practice.
Methods: A meta-analysis was conducted to compare SAC with coiling alone and BAC in the treatment of RIA. Primary outcomes were immediate and follow-up aneurysm occlusion rates, along with perioperative hemorrhagic and ischemic complication rates.
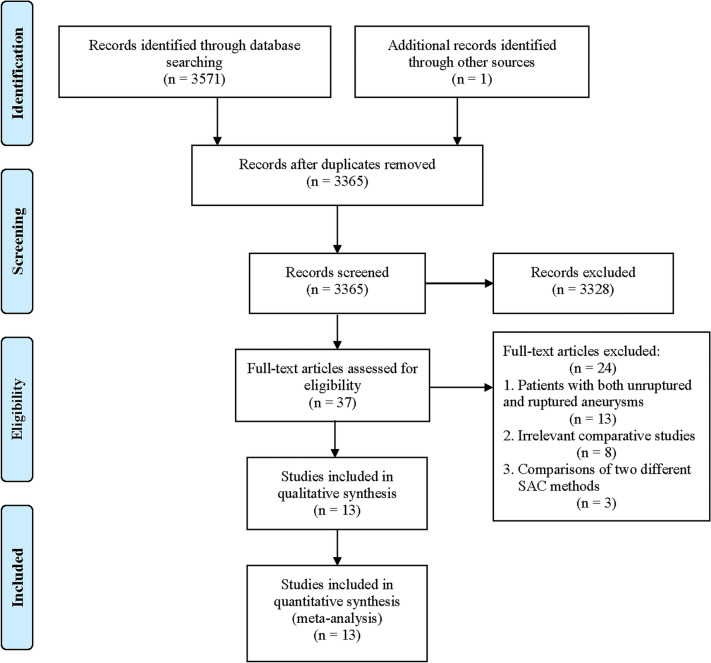
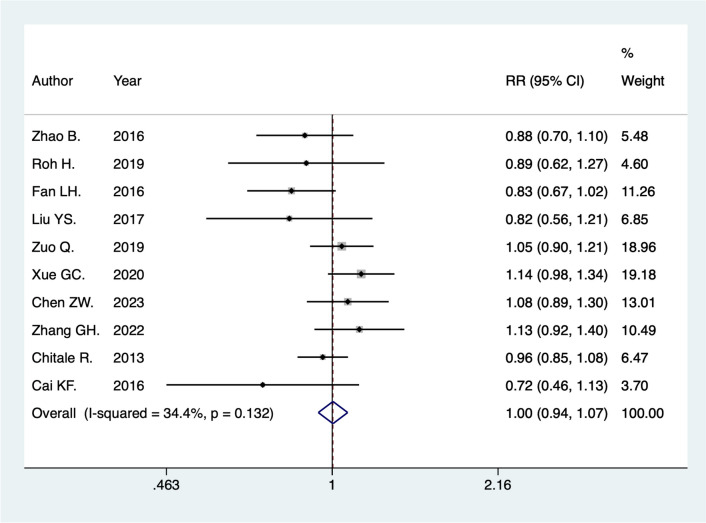
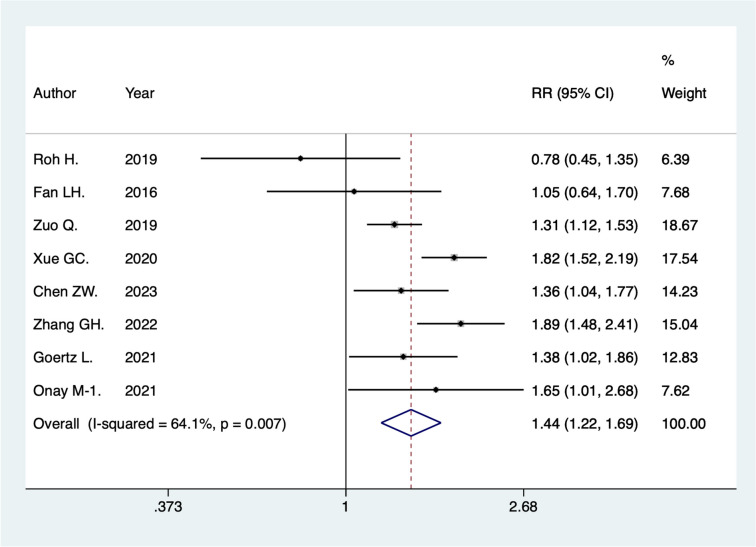
Results: A total of thirteen retrospective cohort studies were included, comprising 3,086 patients, with 1,078 in the SAC group and 2,008 in the non-SAC group. The immediate complete occlusion rates were similar between the SAC and non-SAC groups (59.1% vs. 61.4%; RR = 1.00; 95% CI [0.94, 1.07]; p = 0.92). However, the SAC group demonstrated a significantly higher long-term complete occlusion rate (61.3% vs. 40.6%; RR = 1.44; 95% CI [1.22, 1.69]; p < 0.001). The incidence of ischemic complications was greater in the SAC group (12.2% vs. 10.0%; RR = 1.68; 95% CI [1.37, 2.07]; p < 0.001), as was the incidence of hemorrhagic complications (7.3% vs. 5.1%; RR = 1.55; 95% CI [1.15, 2.08]; p = 0.004). Perioperative mortality was also elevated in the SAC group (6.7% vs. 6.8%; RR = 1.37; 95% CI [1.00, 1.88]; p = 0.048), with a non-significant trend towards higher long-term mortality (9.8% vs. 9.2%; RR = 1.35; 95% CI [0.98, 1.87]; p = 0.068). Functional outcomes at discharge (76.0% vs. 71.0%; RR = 0.97; 95% CI [0.92, 1.02]; p = 0.237), six months (57.8% vs. 60.8%; RR = 0.93; 95% CI [0.81, 1.07]; p = 0.296), and at the last follow-up (RR = 1.01; 95% CI [0.97, 1.06]; p = 0.592) were comparable between the two groups.
Conclusions: SAC significantly improves long-term occlusion rates for RIA compared to non-SAC, despite a higher incidence of complications. Careful patient selection and optimization of antiplatelet therapy may enhance the safety and efficacy of SAC for RIA treatment.
目的:系统评价SAC与非SAC治疗RIA的安全性和有效性,整合高质量研究的证据,指导临床实践。方法:采用meta分析比较SAC与单独盘绕及BAC治疗RIA的疗效。主要结果是即时和随访的动脉瘤闭塞率,以及围手术期出血和缺血性并发症的发生率。结果:共纳入13项回顾性队列研究,包括3086例患者,其中SAC组1078例,非SAC组2008例。即刻完全闭塞率在SAC组和非SAC组之间相似(59.1% vs. 61.4%;rr = 1.00;95% ci [0.94, 1.07];p = 0.92)。然而,SAC组显示出更高的长期完全闭塞率(61.3% vs. 40.6%;rr = 1.44;95% ci [1.22, 1.69];结论:尽管并发症发生率较高,但与非SAC相比,SAC可显著提高RIA的长期闭塞率。谨慎的患者选择和优化抗血小板治疗可以提高SAC治疗RIA的安全性和有效性。
期刊介绍:
Translational Stroke Research covers basic, translational, and clinical studies. The Journal emphasizes novel approaches to help both to understand clinical phenomenon through basic science tools, and to translate basic science discoveries into the development of new strategies for the prevention, assessment, treatment, and enhancement of central nervous system repair after stroke and other forms of neurotrauma.
Translational Stroke Research focuses on translational research and is relevant to both basic scientists and physicians, including but not restricted to neuroscientists, vascular biologists, neurologists, neuroimagers, and neurosurgeons.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


