{"title":"Out-of-Pocket Costs Burden in Marketplace Plans for People With Diabetes.","authors":"Brielle Ruscitti, Caroline Kern, Diana Bowser","doi":"10.1177/11786329241304618","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Affordable Care Act (ACA) aims to expand coverage and increase access to health insurance. Despite the increase of insured individuals, there are a number of concerns about whether coverage and care are affordable. Prior studies document a growing concern with rising premiums and cost-sharing, including deductibles, particularly for those with chronic conditions.</p><p><strong>Objective: </strong>Compare the ACA marketplace plan availability and costs across 17 states for individuals with varying diabetic engagement profiles and their related medical needs.</p><p><strong>Design: </strong>Descriptive Cost Analysis.</p><p><strong>Methods: </strong>Using Healthcare.gov individual state marketplace websites, we utilized a descriptive cost analysis to compare plan availability and costs for premiums, deductibles, co-payments, and co-insurance for an individual aged 63 years old, who was either a non-diabetic, high-engagement or low-engagement diabetic in urban and rural areas. Using the second lowest monthly premium silver plan (the benchmark plan), we calculated annual costs for premiums, co-insurance, co-payments, and deductibles for these individual profiles. We assessed statistical differences between health care component costs, within and across urban and rural areas, using <i>t</i>-tests.</p><p><strong>Results: </strong>The findings highlight within and across states, individuals with diabetes, particularly low-engagement diabetics, spend a significantly higher percent of their income on additional health care costs, above their premium, than non-diabetic individuals. In some states, low-engagement diabetic patients spend upwards of 3 times more than high-engagement diabetic patients, highlighting an additional cost burden. For low-engagement diabetics, deductibles are driving health care spending with an average of 59% of health care spending coming from deductible payments. Results do not show statistically different costs across urban and rural diabetic patients.</p><p><strong>Conclusion: </strong>Despite the ACA's success, results highlight variation in plan availability across states and disproportionate cost burden placed on moderate income individuals, especially related to deductible, and co-payments for those with chronic diseases.</p>","PeriodicalId":12876,"journal":{"name":"Health Services Insights","volume":"17 ","pages":"11786329241304618"},"PeriodicalIF":2.5000,"publicationDate":"2024-12-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11613290/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11786329241304618","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Affordable Care Act (ACA) aims to expand coverage and increase access to health insurance. Despite the increase of insured individuals, there are a number of concerns about whether coverage and care are affordable. Prior studies document a growing concern with rising premiums and cost-sharing, including deductibles, particularly for those with chronic conditions.
Objective: Compare the ACA marketplace plan availability and costs across 17 states for individuals with varying diabetic engagement profiles and their related medical needs.
Design: Descriptive Cost Analysis.
Methods: Using Healthcare.gov individual state marketplace websites, we utilized a descriptive cost analysis to compare plan availability and costs for premiums, deductibles, co-payments, and co-insurance for an individual aged 63 years old, who was either a non-diabetic, high-engagement or low-engagement diabetic in urban and rural areas. Using the second lowest monthly premium silver plan (the benchmark plan), we calculated annual costs for premiums, co-insurance, co-payments, and deductibles for these individual profiles. We assessed statistical differences between health care component costs, within and across urban and rural areas, using t-tests.
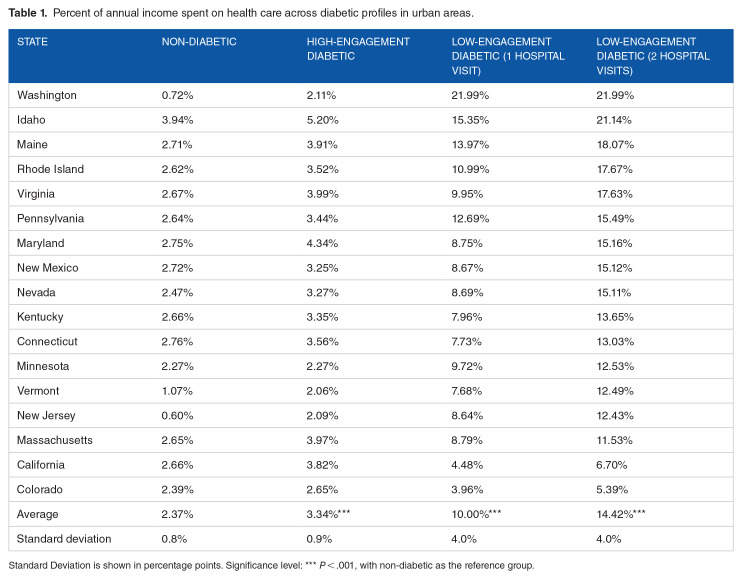
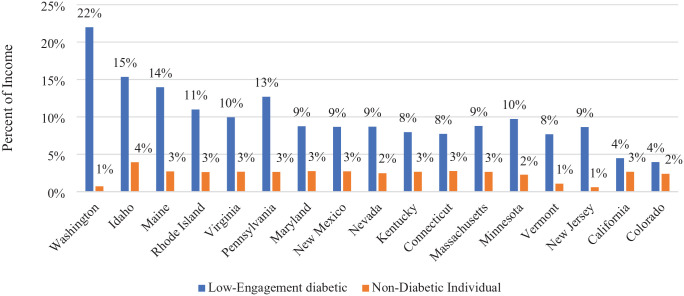
Results: The findings highlight within and across states, individuals with diabetes, particularly low-engagement diabetics, spend a significantly higher percent of their income on additional health care costs, above their premium, than non-diabetic individuals. In some states, low-engagement diabetic patients spend upwards of 3 times more than high-engagement diabetic patients, highlighting an additional cost burden. For low-engagement diabetics, deductibles are driving health care spending with an average of 59% of health care spending coming from deductible payments. Results do not show statistically different costs across urban and rural diabetic patients.
Conclusion: Despite the ACA's success, results highlight variation in plan availability across states and disproportionate cost burden placed on moderate income individuals, especially related to deductible, and co-payments for those with chronic diseases.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


