{"title":"Pelvic/Sacral Chondrosarcoma with Brain Metastasis: A Case Report.","authors":"Catalina Herrán-Fonseca, Jorge Luis Vargas-Rojas, Ramón Alejandro Andreu-Atuesta, Sergio Andrés Salgado-Rueda","doi":"10.1159/000541620","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Chondrosarcomas are cartilaginous tumors primarily known for metastasizing to the lungs and bones. Their spread to the central nervous system is infrequent.</p><p><strong>Case presentation: </strong>We present the case of a 32-year-old woman with a history of pelvic/sacral grade III chondrosarcoma (L4-S2; T3N0MX; Ki67; 30%), who underwent surgical resection and radiotherapy. She presented to the emergency department with a 2-day history of thunderclap headache accompanied by fever and chills. Computed axial tomography (CT) scan revealed a left occipital intraparenchymal lesion, subsequently confirmed as suggestive of a neoplastic lesion on magnetic resonance imaging. Ten days after admission, she experienced a two-minute generalized tonic-clonic seizure episode, followed by postictal stupor, tachycardia, hypertension, and anisochoric pupils. A follow-up CT scan demonstrated progression of the metastatic lesion, with evidence of uncal and foraminal herniation. Compression of the cardiorespiratory center at the bulbar level led to her death.</p><p><strong>Conclusion: </strong>This case report offers insight into the clinical presentation, behavior, and prognosis of a metastatic brain lesion derived from grade III chondrosarcoma. It is important to correlate the patient's medical history with imaging findings to achieve an accurate diagnosis, especially in situations where biopsy may not be feasible.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"17 1","pages":"1335-1341"},"PeriodicalIF":0.7000,"publicationDate":"2024-12-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11611304/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000541620","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Chondrosarcomas are cartilaginous tumors primarily known for metastasizing to the lungs and bones. Their spread to the central nervous system is infrequent.
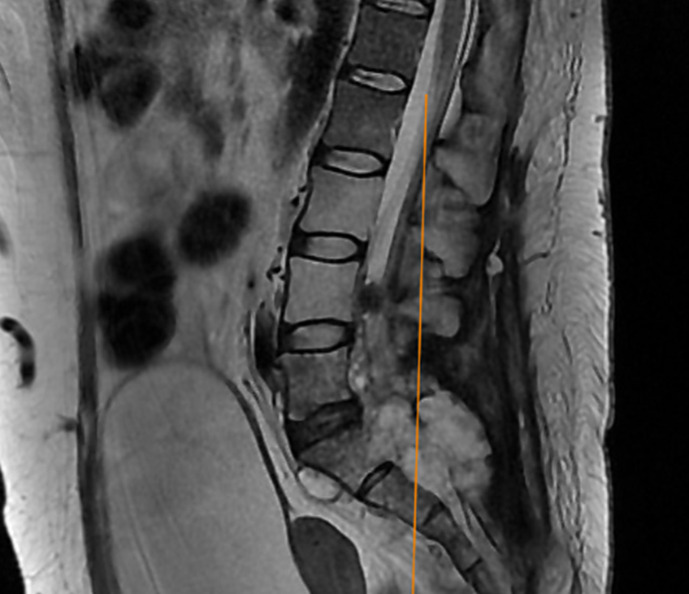
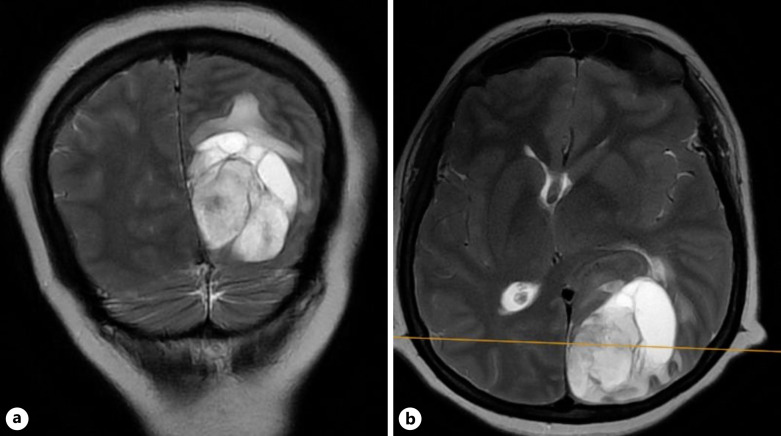
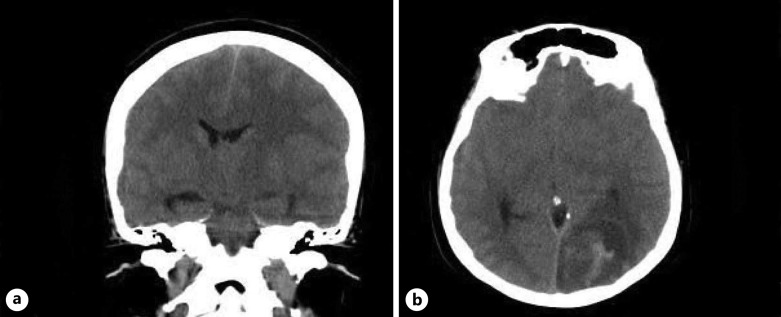
Case presentation: We present the case of a 32-year-old woman with a history of pelvic/sacral grade III chondrosarcoma (L4-S2; T3N0MX; Ki67; 30%), who underwent surgical resection and radiotherapy. She presented to the emergency department with a 2-day history of thunderclap headache accompanied by fever and chills. Computed axial tomography (CT) scan revealed a left occipital intraparenchymal lesion, subsequently confirmed as suggestive of a neoplastic lesion on magnetic resonance imaging. Ten days after admission, she experienced a two-minute generalized tonic-clonic seizure episode, followed by postictal stupor, tachycardia, hypertension, and anisochoric pupils. A follow-up CT scan demonstrated progression of the metastatic lesion, with evidence of uncal and foraminal herniation. Compression of the cardiorespiratory center at the bulbar level led to her death.
Conclusion: This case report offers insight into the clinical presentation, behavior, and prognosis of a metastatic brain lesion derived from grade III chondrosarcoma. It is important to correlate the patient's medical history with imaging findings to achieve an accurate diagnosis, especially in situations where biopsy may not be feasible.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


