{"title":"Late Diagnostic Clues in Rapidly Progressing Probable Heidenhain Variant of Creutzfeldt-Jakob Disease.","authors":"Rahul Gaini, Julia Denniss, Elijah Lackey","doi":"10.1155/crnm/4618310","DOIUrl":null,"url":null,"abstract":"<p><p>Presenting symptoms of sporadic Creutzfeldt-Jakob disease (sCJD) are variable, and as imaging and EEG may be normal in the early to middle stages of the disease process, serial testing is vital when there is clinical suspicion for sCJD. We present a case of probable Heidenhain variant of sCJD (HvCJD) with notable rapid progression. A 72-year-old woman presented with neurological decline following new-onset visual changes. Over the course of 3 weeks, she developed ataxia followed by paranoia, memory impairment, and visual hallucinations. An extensive workup from 1 week prior at an outside hospital was unrevealing and included two magnetic resonance imaging (MRI) studies read as normal and an EEG without periodic sharp wave complexes. Repeat of imaging at our hospital showed cortical restricted diffusion in the right occipital lobe. In combination with new periodic sharp wave complexes visualized on prolonged EEG, concern was raised for sCJD. Palliative care was consulted early in the hospitalization, and the patient was transitioned to comfort care and discharged 3 days after admission. She declined quickly and passed away at home within a week, one day before her send out CSF sample resulted with a positive real-time quaking-induced conversion (RT-QuiC) and markedly elevated T-tau protein and 14-3-3 gamma. As there is no treatment for this fatal disease, palliative engagement and discussion of goals of care in cases of CJD is critical in providing compassionate care for the patient and their family. High clinical suspicion warrants discussion of comfort care measures even prior to confirmation with RT-QuiC.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2024 ","pages":"4618310"},"PeriodicalIF":0.9000,"publicationDate":"2024-11-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11614507/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crnm/4618310","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
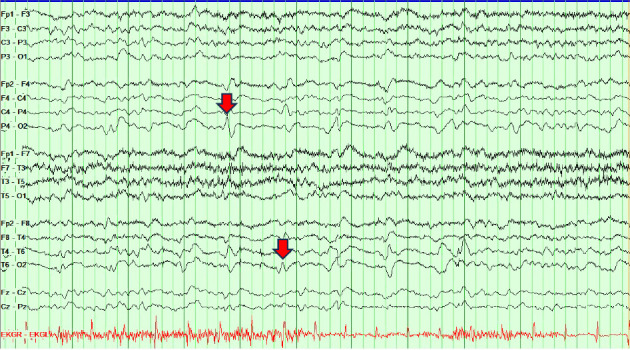
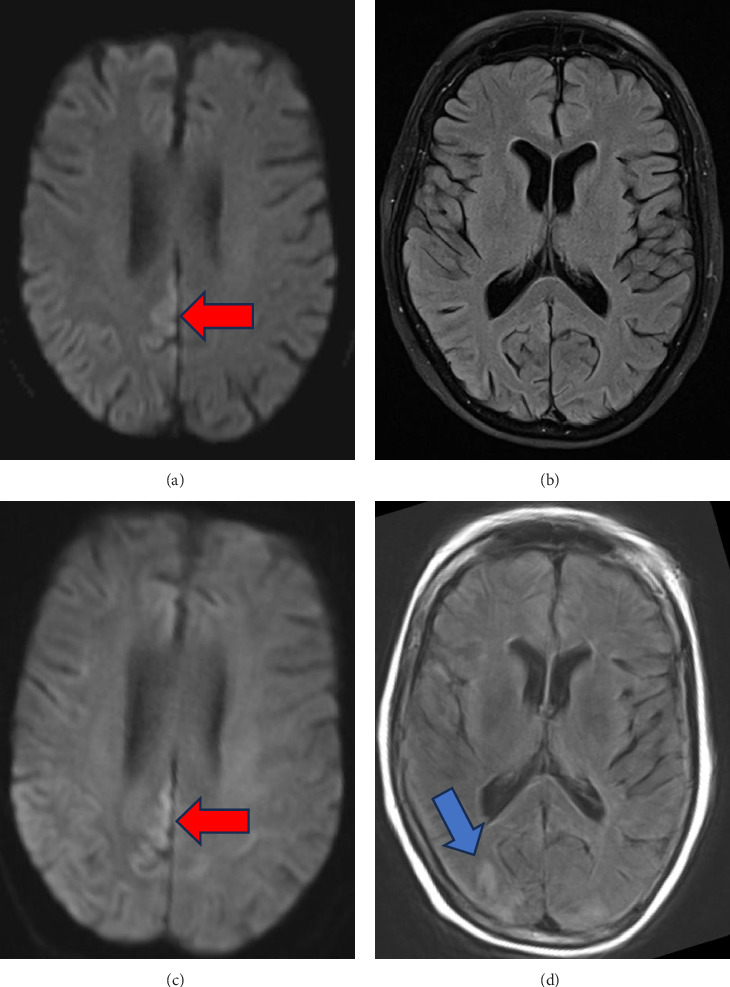
Presenting symptoms of sporadic Creutzfeldt-Jakob disease (sCJD) are variable, and as imaging and EEG may be normal in the early to middle stages of the disease process, serial testing is vital when there is clinical suspicion for sCJD. We present a case of probable Heidenhain variant of sCJD (HvCJD) with notable rapid progression. A 72-year-old woman presented with neurological decline following new-onset visual changes. Over the course of 3 weeks, she developed ataxia followed by paranoia, memory impairment, and visual hallucinations. An extensive workup from 1 week prior at an outside hospital was unrevealing and included two magnetic resonance imaging (MRI) studies read as normal and an EEG without periodic sharp wave complexes. Repeat of imaging at our hospital showed cortical restricted diffusion in the right occipital lobe. In combination with new periodic sharp wave complexes visualized on prolonged EEG, concern was raised for sCJD. Palliative care was consulted early in the hospitalization, and the patient was transitioned to comfort care and discharged 3 days after admission. She declined quickly and passed away at home within a week, one day before her send out CSF sample resulted with a positive real-time quaking-induced conversion (RT-QuiC) and markedly elevated T-tau protein and 14-3-3 gamma. As there is no treatment for this fatal disease, palliative engagement and discussion of goals of care in cases of CJD is critical in providing compassionate care for the patient and their family. High clinical suspicion warrants discussion of comfort care measures even prior to confirmation with RT-QuiC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


