Giorgio Imbrogno, Andrea Lorenzi, Roberto Borloni, Riccardo Scaini, Tiziano Testori, Giovanni Felisati, Alberto Maria Saibene, John R. Craig
{"title":"Maxillary Sinusitis Following Orthognathic Surgery: Should It Be Considered Odontogenic Sinusitis?","authors":"Giorgio Imbrogno, Andrea Lorenzi, Roberto Borloni, Riccardo Scaini, Tiziano Testori, Giovanni Felisati, Alberto Maria Saibene, John R. Craig","doi":"10.1002/ccr3.9654","DOIUrl":null,"url":null,"abstract":"<p>Maxillary sinusitis is a recognized complication following dental procedures, but its occurrence after orthognathic surgery, such as Le Fort osteotomies, remains less documented. This case report presents a 58-year-old female who developed unilateral maxillary sinusitis 23 years post-orthognathic surgery. The patient was asymptomatic, aside from occasional cacosmia, and was incidentally found to have sinus opacification on a computed tomography (CT) scan performed for implant-prosthetic rehabilitation. Nasal endoscopy revealed purulence and mucosal edema, prompting endoscopic sinus surgery (ESS). Intraoperatively, purulent material and fungal debris were removed from the maxillary sinus, confirming bacterial sinusitis with a concurrent fungal ball. <i>S. salivarius</i> and <i>Klebsiella</i> species were identified from the cultures. The patient's condition improved following the removal of both the sinus contents and the retained titanium plates and screws. This case underscores the potential for maxillary sinusitis to develop long after orthognathic surgery, particularly in the presence of retained dental hardware. It highlights the importance of thorough imaging and endoscopic evaluation in patients with a history of dental or facial surgeries presenting with sinonasal symptoms. Additionally, it raises questions about the role of retained hardware in the persistence or recurrence of infection and the possible association with fungal ball formation. The need for further research to establish guidelines for the management of sinusitis in such contexts, particularly regarding the removal of facial hardware, is emphasized.</p>","PeriodicalId":10327,"journal":{"name":"Clinical Case Reports","volume":"12 12","pages":""},"PeriodicalIF":0.6000,"publicationDate":"2024-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccr3.9654","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ccr3.9654","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
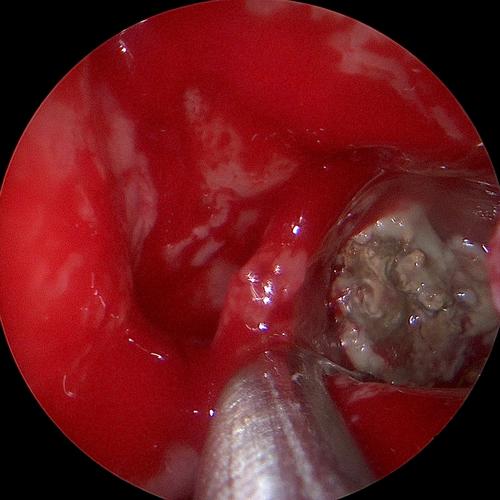
Maxillary sinusitis is a recognized complication following dental procedures, but its occurrence after orthognathic surgery, such as Le Fort osteotomies, remains less documented. This case report presents a 58-year-old female who developed unilateral maxillary sinusitis 23 years post-orthognathic surgery. The patient was asymptomatic, aside from occasional cacosmia, and was incidentally found to have sinus opacification on a computed tomography (CT) scan performed for implant-prosthetic rehabilitation. Nasal endoscopy revealed purulence and mucosal edema, prompting endoscopic sinus surgery (ESS). Intraoperatively, purulent material and fungal debris were removed from the maxillary sinus, confirming bacterial sinusitis with a concurrent fungal ball. S. salivarius and Klebsiella species were identified from the cultures. The patient's condition improved following the removal of both the sinus contents and the retained titanium plates and screws. This case underscores the potential for maxillary sinusitis to develop long after orthognathic surgery, particularly in the presence of retained dental hardware. It highlights the importance of thorough imaging and endoscopic evaluation in patients with a history of dental or facial surgeries presenting with sinonasal symptoms. Additionally, it raises questions about the role of retained hardware in the persistence or recurrence of infection and the possible association with fungal ball formation. The need for further research to establish guidelines for the management of sinusitis in such contexts, particularly regarding the removal of facial hardware, is emphasized.
期刊介绍:
Clinical Case Reports is different from other case report journals. Our aim is to directly improve global health and increase clinical understanding using case reports to convey important best practice information. We welcome case reports from all areas of Medicine, Nursing, Dentistry, and Veterinary Science and may include: -Any clinical case or procedure which illustrates an important best practice teaching message -Any clinical case or procedure which illustrates the appropriate use of an important clinical guideline or systematic review. As well as: -The management of novel or very uncommon diseases -A common disease presenting in an uncommon way -An uncommon disease masquerading as something more common -Cases which expand understanding of disease pathogenesis -Cases where the teaching point is based on an error -Cases which allow us to re-think established medical lore -Unreported adverse effects of interventions (drug, procedural, or other).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


