{"title":"A systematic review of economic evaluation of healthcare associated infection prevention and control interventions in long term care facilities.","authors":"Eric Nguemeleu Tchouaket, Fatima El-Mousawi, Stephanie Robins, Katya Kruglova, Catherine Séguin, Kelley Kilpatrick, Maripier Jubinville, Suzanne Leroux, Idrissa Beogo, Drissa Sia","doi":"10.1186/s13561-024-00582-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Healthcare-associated infections (HCAI) are common in long-term care facilities (LTCF) and cause significant burden. Infection prevention and control (IPC) measures include the clinical best practices (CBP) of hand hygiene, hygiene and sanitation, screening, and basic and additional precautions. Few studies demonstrate their cost-effectiveness in LTCF, and those that do, largely focus on one CBP. An overarching synthesis of IPC economic analyses in this context is warranted. The aim of this paper is to conduct a systematic review of economic evaluations of CBP applied in LTCF.</p><p><strong>Methods: </strong>We twice queried CINAHL, Cochrane, EconLit, Embase, Medline, Web of Science and Scopus for studies published in the last three decades of economic evaluations of CBP in LTCF. We included controlled and randomized clinical trials, cohort, longitudinal, follow-up, prospective, retrospective, cross-sectional, and simulations studies, as well as those based on mathematical or statistical modelling. Two reviewers conducted study selection, data extraction, and quality assessment of studies. We applied discounting rates of 3%, 5% and 8%, and presented all costs in 2022 Canadian dollars. The protocol of this review was registered with Research Registry (reviewregistry1210) and published in BMC Systematic Reviews.</p><p><strong>Findings: </strong>We found 3,331 records and then 822 records; ten studies were retained. The economic analyses described were cost-minimization (n = 1), cost-benefit (n = 1), cost-savings (n = 2), cost-utility (n = 2) and cost-effectiveness which included cost-utility and cost-benefit analyses (n = 4). Four studies were high quality, three were moderate, and three were low quality. Inter-rater agreement for quality assessment was 91⋅7%. All studies (n = 10) demonstrated that CBP associated with IPC are clinically effective in LTCF and many (n = 6) demonstrated their cost effectiveness.</p><p><strong>Interpretation: </strong>Ongoing economic evaluation research of IPC remains essential to underpin healthcare policy choices guided by empirical evidence for LTCF residents and staff.</p>","PeriodicalId":46936,"journal":{"name":"Health Economics Review","volume":"14 1","pages":"101"},"PeriodicalIF":3.3000,"publicationDate":"2024-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11605862/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Economics Review","FirstCategoryId":"96","ListUrlMain":"https://doi.org/10.1186/s13561-024-00582-8","RegionNum":3,"RegionCategory":"经济学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Healthcare-associated infections (HCAI) are common in long-term care facilities (LTCF) and cause significant burden. Infection prevention and control (IPC) measures include the clinical best practices (CBP) of hand hygiene, hygiene and sanitation, screening, and basic and additional precautions. Few studies demonstrate their cost-effectiveness in LTCF, and those that do, largely focus on one CBP. An overarching synthesis of IPC economic analyses in this context is warranted. The aim of this paper is to conduct a systematic review of economic evaluations of CBP applied in LTCF.
Methods: We twice queried CINAHL, Cochrane, EconLit, Embase, Medline, Web of Science and Scopus for studies published in the last three decades of economic evaluations of CBP in LTCF. We included controlled and randomized clinical trials, cohort, longitudinal, follow-up, prospective, retrospective, cross-sectional, and simulations studies, as well as those based on mathematical or statistical modelling. Two reviewers conducted study selection, data extraction, and quality assessment of studies. We applied discounting rates of 3%, 5% and 8%, and presented all costs in 2022 Canadian dollars. The protocol of this review was registered with Research Registry (reviewregistry1210) and published in BMC Systematic Reviews.
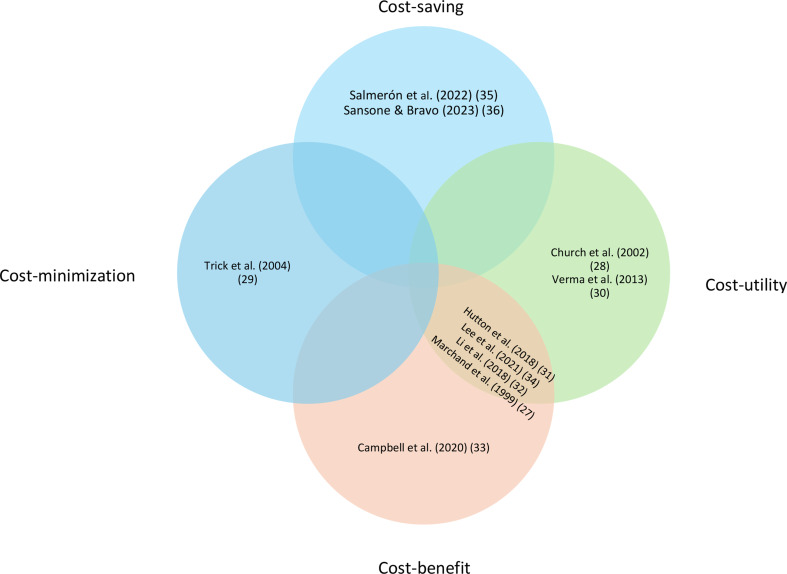
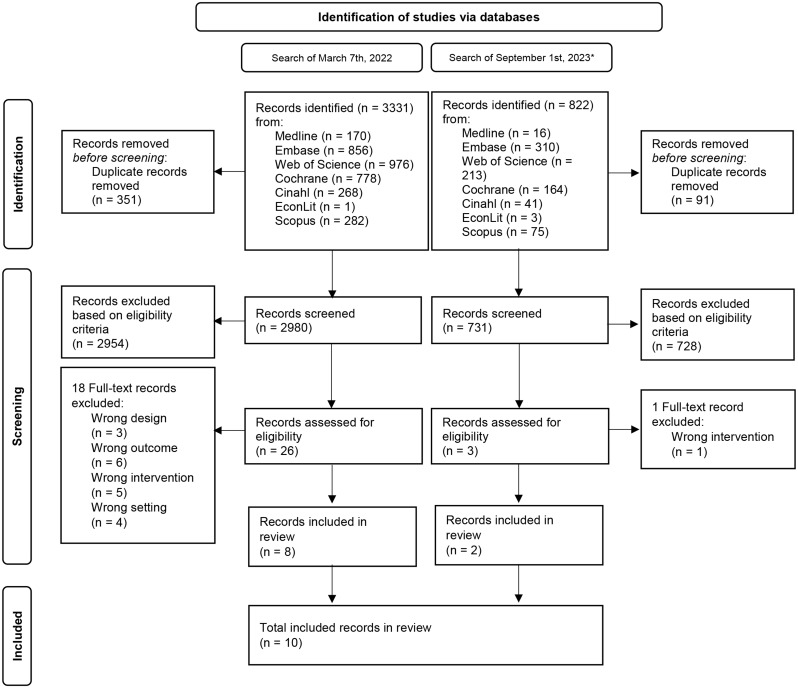
Findings: We found 3,331 records and then 822 records; ten studies were retained. The economic analyses described were cost-minimization (n = 1), cost-benefit (n = 1), cost-savings (n = 2), cost-utility (n = 2) and cost-effectiveness which included cost-utility and cost-benefit analyses (n = 4). Four studies were high quality, three were moderate, and three were low quality. Inter-rater agreement for quality assessment was 91⋅7%. All studies (n = 10) demonstrated that CBP associated with IPC are clinically effective in LTCF and many (n = 6) demonstrated their cost effectiveness.
Interpretation: Ongoing economic evaluation research of IPC remains essential to underpin healthcare policy choices guided by empirical evidence for LTCF residents and staff.
期刊介绍:
Health Economics Review is an international high-quality journal covering all fields of Health Economics. A broad range of theoretical contributions, empirical studies and analyses of health policy with a health economic focus will be considered for publication. Its scope includes macro- and microeconomics of health care financing, health insurance and reimbursement as well as health economic evaluation, health services research and health policy analysis. Further research topics are the individual and institutional aspects of health care management and the growing importance of health care in developing countries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


