Alberto Palazzuoli, Filippo Pirrotta, Alessandra Cartocci, Elvira Delcuratolo, Frank Loyd Dini, Michele Correale, Giuseppe Dattilo, Daniele Masarone, Laura Scelsi, Stefano Ghio, Carlo Gabriele Tocchetti, Valentina Mercurio, Natale Daniele Brunetti, Savina Nodari, Francesco Barillà, Giuseppe Ambrosio, Erberto Carluccio
{"title":"Effects of sacubitril/valsartan on renal function and outcome in patients with heart failure and reduced ejection fraction: an Italian cohort study.","authors":"Alberto Palazzuoli, Filippo Pirrotta, Alessandra Cartocci, Elvira Delcuratolo, Frank Loyd Dini, Michele Correale, Giuseppe Dattilo, Daniele Masarone, Laura Scelsi, Stefano Ghio, Carlo Gabriele Tocchetti, Valentina Mercurio, Natale Daniele Brunetti, Savina Nodari, Francesco Barillà, Giuseppe Ambrosio, Erberto Carluccio","doi":"10.1177/17539447241285136","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sacubitril/valsartan (S/V) is a cornerstone treatment for heart failure (HF). Beneficial effects on hospitalization rates, mortality, and left ventricular remodeling have been observed in patients with heart failure and reduced ejection fraction (HFrEF). Despite the positive results, the influence of S/V on renal function during long-term follow-up has received little attention.</p><p><strong>Aims: </strong>We investigated the long-term effects of S/V therapy on renal function in a large cohort of patients with HFrEF. Additionally, we examined the effects of the drug in patients with chronic kidney disease (CKD) compared to those with preserved renal function and identified primary risk characteristics.</p><p><strong>Methods: </strong>We studied 776 outpatients with HFrEF and left ventricular ejection fraction (LVEF) <40% from an observational registry of the Italian Society of Cardiology, all receiving optimized standard-of-care therapy with S/V. The patients were included in a multicentric open-label registry from 11 Italian academic hospitals. Kidney function was evaluated at baseline, after 6 months of S/V, and at 4 years. Patients were followed-up through periodic clinical visits.</p><p><strong>Results: </strong>During a 48-month follow-up period, 591 patients remained stable and 185 patients (24%) experienced adverse events (85 deaths and 126 hospitalizations). S/V therapy marginally affects renal function during the follow-up period (estimated glomerular filtration rate (eGFR) at baseline 72.01 vs eGFR at follow-up 70.38 ml/min/m<sup>2</sup>, <i>p</i> = 0.01; and creatinine was 1.06 at baseline vs 1.10 at follow-up, <i>p</i> < 0.04). Among patients who maintained preserved renal function, 35% were in Dose 3 and 10% dropped out of S/V therapy (<i>p</i> < 0.006). Univariate analysis showed that Drop-out of S/V (HR 2.73 [2.01, 3.71], <i>p</i> < 0.001), history of previous HF hospitalization (HR 1.75 [1.30, 2.36], <i>p</i> < 0.001), advanced NYHA class (HR 2.14 [1.60, 2.86], <i>p</i> < 0.001), NT-proBNP values >1000 pg/ml (HR 1.95[1.38, 2.77], <i>p</i> < 0.001), furosemide dose >50 mg (HR 2.04 [1.48, 2.82], <i>p</i> < 0.001), and creatinine values >1.5 mg/dl occurred during follow-up (HR 1.74 [1.24, 2.43], <i>p</i> < 0.001) were linked to increased risk. At multivariable analysis, increased doses of loop diuretics, advanced NYHA class, creatinine >1.5 mg/dl, and atrial fibrillation were independent predictors of adverse events.</p><p><strong>Conclusion: </strong>Long-term S/V therapy is associated with improved outcomes and renal protection in patients with HFrEF. This effect is more pronounced in patients who tolerate escalating doses. The positive effects of the drug are maintained in both CKD and preserved renal function. Future research may study the safety and underlying causes of current protection.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":"18 ","pages":"17539447241285136"},"PeriodicalIF":2.2000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11607766/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17539447241285136","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sacubitril/valsartan (S/V) is a cornerstone treatment for heart failure (HF). Beneficial effects on hospitalization rates, mortality, and left ventricular remodeling have been observed in patients with heart failure and reduced ejection fraction (HFrEF). Despite the positive results, the influence of S/V on renal function during long-term follow-up has received little attention.
Aims: We investigated the long-term effects of S/V therapy on renal function in a large cohort of patients with HFrEF. Additionally, we examined the effects of the drug in patients with chronic kidney disease (CKD) compared to those with preserved renal function and identified primary risk characteristics.
Methods: We studied 776 outpatients with HFrEF and left ventricular ejection fraction (LVEF) <40% from an observational registry of the Italian Society of Cardiology, all receiving optimized standard-of-care therapy with S/V. The patients were included in a multicentric open-label registry from 11 Italian academic hospitals. Kidney function was evaluated at baseline, after 6 months of S/V, and at 4 years. Patients were followed-up through periodic clinical visits.
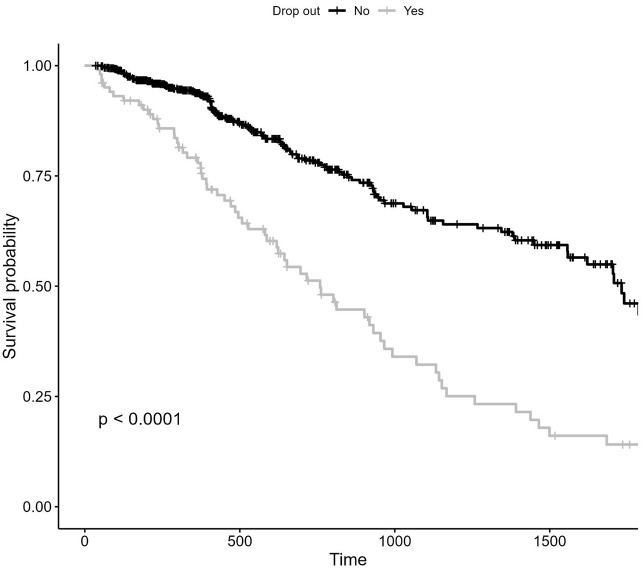
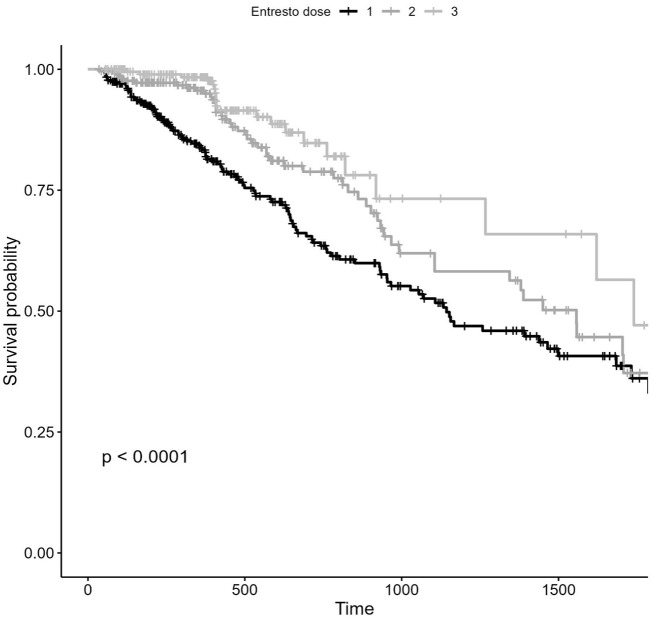
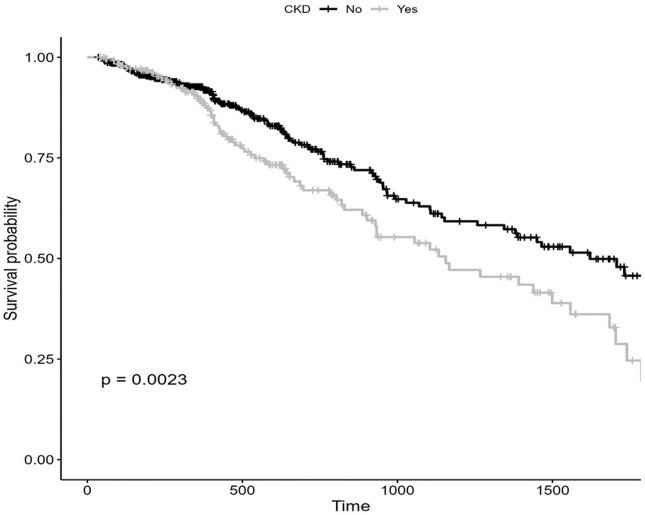
Results: During a 48-month follow-up period, 591 patients remained stable and 185 patients (24%) experienced adverse events (85 deaths and 126 hospitalizations). S/V therapy marginally affects renal function during the follow-up period (estimated glomerular filtration rate (eGFR) at baseline 72.01 vs eGFR at follow-up 70.38 ml/min/m2, p = 0.01; and creatinine was 1.06 at baseline vs 1.10 at follow-up, p < 0.04). Among patients who maintained preserved renal function, 35% were in Dose 3 and 10% dropped out of S/V therapy (p < 0.006). Univariate analysis showed that Drop-out of S/V (HR 2.73 [2.01, 3.71], p < 0.001), history of previous HF hospitalization (HR 1.75 [1.30, 2.36], p < 0.001), advanced NYHA class (HR 2.14 [1.60, 2.86], p < 0.001), NT-proBNP values >1000 pg/ml (HR 1.95[1.38, 2.77], p < 0.001), furosemide dose >50 mg (HR 2.04 [1.48, 2.82], p < 0.001), and creatinine values >1.5 mg/dl occurred during follow-up (HR 1.74 [1.24, 2.43], p < 0.001) were linked to increased risk. At multivariable analysis, increased doses of loop diuretics, advanced NYHA class, creatinine >1.5 mg/dl, and atrial fibrillation were independent predictors of adverse events.
Conclusion: Long-term S/V therapy is associated with improved outcomes and renal protection in patients with HFrEF. This effect is more pronounced in patients who tolerate escalating doses. The positive effects of the drug are maintained in both CKD and preserved renal function. Future research may study the safety and underlying causes of current protection.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


