{"title":"The outcome of thrombotic microangiopathy in kidney transplant recipients.","authors":"Kanza Haq, Shanshan Lin, Alana Dasgupta, Zainab Obaidi, Serena Bagnasco, Umberto Maggiore, Nada Alachkar","doi":"10.1186/s12882-024-03846-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The outcome of kidney transplant recipients with a history of complement-mediated thrombotic microangiopathy (cTMA) and those who develop post-transplant de novo TMA (dnTMA) is largely unknown.</p><p><strong>Methods: </strong>We retrospectively studied all kidney transplant recipients with end-stage kidney disease secondary to cTMA and those who developed dnTMA, between Jan 2000 and Dec 2020 in our center.</p><p><strong>Results: </strong>We identified 134 patients, 22 with cTMA and 112 had dnTMA. Patients with cTMA were younger at the time of TMA diagnosis (age at diagnosis, 28.9 ± 16.3. vs 46.5 ± 16.0 years; P < 0.001). T-cell mediated rejection, borderline rejection, and calcineurin inhibitor toxicity were more prevalent in the first kidney transplant biopsy (P < 0.05) in the dnTMA group, and antibody-mediated rejection was more prevalent in anytime-biopsy (P = 0.027). After adjusting for potential confounders, cTMA was associated with a sixfold increase in the hazard of transplant failure during the first-year post-transplant (adjusted hazard ratio (aHR): 6.37 [95%CI: 2.17 to18.68; P = 0.001]; the aHR decreased by 0.87 (95% CI: 0.76 to 0.99: P = 0.033) per year elapsed since transplantation. Long-term allograft survival was similar in both groups.</p><p><strong>Conclusion: </strong>Post kidney transplant TMA is an important cause of poor allograft survival. More studies are needed to enhance our understanding and management of this disorder.</p>","PeriodicalId":9089,"journal":{"name":"BMC Nephrology","volume":"25 1","pages":"433"},"PeriodicalIF":2.4000,"publicationDate":"2024-11-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11606107/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12882-024-03846-x","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The outcome of kidney transplant recipients with a history of complement-mediated thrombotic microangiopathy (cTMA) and those who develop post-transplant de novo TMA (dnTMA) is largely unknown.
Methods: We retrospectively studied all kidney transplant recipients with end-stage kidney disease secondary to cTMA and those who developed dnTMA, between Jan 2000 and Dec 2020 in our center.
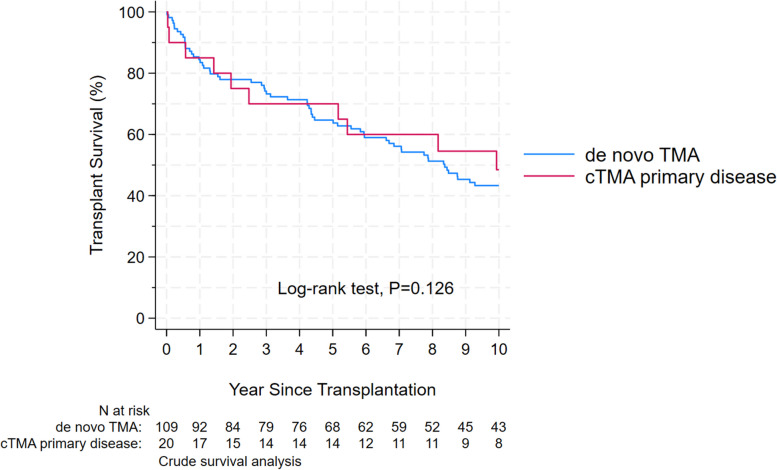
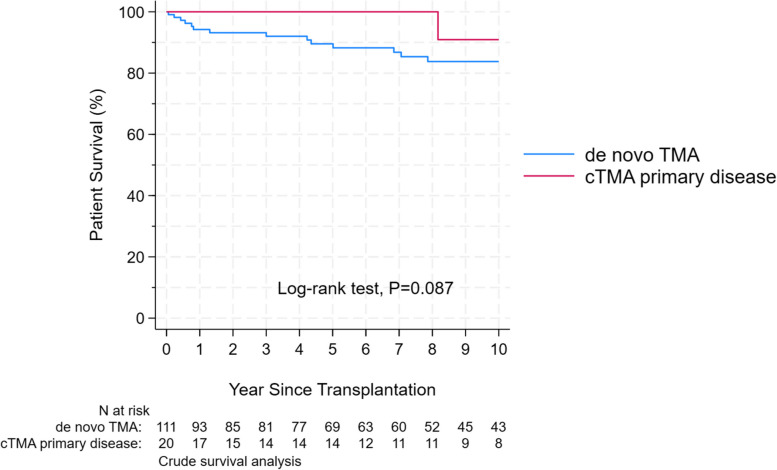
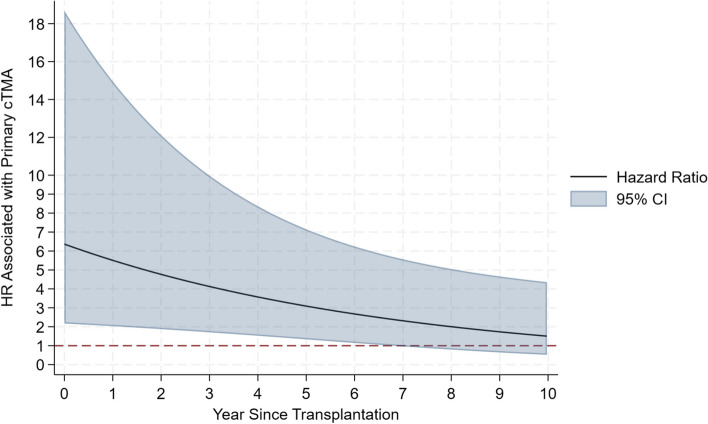
Results: We identified 134 patients, 22 with cTMA and 112 had dnTMA. Patients with cTMA were younger at the time of TMA diagnosis (age at diagnosis, 28.9 ± 16.3. vs 46.5 ± 16.0 years; P < 0.001). T-cell mediated rejection, borderline rejection, and calcineurin inhibitor toxicity were more prevalent in the first kidney transplant biopsy (P < 0.05) in the dnTMA group, and antibody-mediated rejection was more prevalent in anytime-biopsy (P = 0.027). After adjusting for potential confounders, cTMA was associated with a sixfold increase in the hazard of transplant failure during the first-year post-transplant (adjusted hazard ratio (aHR): 6.37 [95%CI: 2.17 to18.68; P = 0.001]; the aHR decreased by 0.87 (95% CI: 0.76 to 0.99: P = 0.033) per year elapsed since transplantation. Long-term allograft survival was similar in both groups.
Conclusion: Post kidney transplant TMA is an important cause of poor allograft survival. More studies are needed to enhance our understanding and management of this disorder.
期刊介绍:
BMC Nephrology is an open access journal publishing original peer-reviewed research articles in all aspects of the prevention, diagnosis and management of kidney and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


